Chronic viral hepatitis with (HSS) - inflammatory disease The liver caused by the hepatitis C virus (NSV), lasting 6 months or more and capable of cirrhosis or be associated with cirrhosis. It is believed that the following HCV genotypes should be distinguished for the purposes of clinical practice: 1a, 1B, 2A, 2B and 3A. 1b and 3a genotypes prevail in Russia. The disease is characterized by a sequential change of acute, latent phases and a phase of reactivation, liver cirrhosis and hepatocellular carcinoma. In the sharp phase of 10-15%, complete elimination of the virus and recovery is possible. The latent phase is more often registered with women as "chronic virusism". The presence in the blood of Nsv RNa does not necessarily indicate a virus replication, since the pathological changes in the liver tissue may be absent or be minimal. The presence of a virus in the blood in the absence of histological changes in the bioptate implies infection with invisible strains of the virus, the body tolerance to the NSV, as well as the possible extratectic replication of the virus.
According to the criteria for American consensus on hepatitis C from 2000, the optimal approaches have been developed for diagnosing and monitoring the disease. Tests with which antibodies to the virus are determined, the ELIS method includes sets containing NSV antigens from Core and non-structural genes, and recombinant immunobloting methods (RIBA). Aimensional amplification tests comprising a polymerase chain reaction (PCR) or transcriptional-indirect amplification (TOA) are designed to identify HCV RNA. A biopsy can give a histological characteristic of liver damage, but not diagnose NSV infection. In patients with positive results in the IFA, the presence of a persistent NSV infection must be confirmed by the method of qualitative definition of NSV RNA. Testing HCV RNA (or viral load) levels with such methods such as quantitative PCR (KPCR) or branched DNA amplification test gives accurate information. The quantitative definition of the virus gives important information about the effectiveness of the treatment.
For laboratory confirmation of the diagnosis, it is necessary to investigate the blood by the ELISA method for the presence of antibodies to the NSV and the activity of the Alat. Antibodies to NSV can be found not only in the blood, but also to enter the CEC. The degree of severity of inflammation activity, the stage of fibrosis or the presence of a cirrhosis already formed can predict response to interferonotherapy. All patients with HGS are potential candidates for antiviral therapy (PVT). An indication for the conduct of etiopathogenetic therapy is moderate or severe necrotic inflammation and / or fibrosis of the liver under the levels of HCV RNA in the blood serum. The target of therapy for HBGS is the eradication of the virus, slowing the progression of the disease, improving the histological pattern of the liver, reducing the risk of the development of the ICC and improving the quality of life associated with the state of health.
RCRZ (Republican Center for Health Development MD RK)
Version: Clinical Protocols MOR RK - 2015
Chronic viral hepatitis C (B18.2)
Gastroenterology
general information
Short description
Recommended
Expert Council
RGP on PFV "Republican Center
Health Development »
Ministry of Health
and social development
Republic of Kazakhstan
from "10" December 2015
Minutes No. 19.
Protocol name:Chronic viral hepatitis with adults
Chronic hepatitis C. - The liver disease caused by the hepatitis C virus with a duration of 6 or more months. In 10 - 40% of cases, chronic hepatitis C is progressing to the liver cirrhosis, and in 5% of cases - to hepatocellular carcinoma (more often in patients with cirrhosis or pronounced fibrosis)
Protocol code:
MKB -10 codes:
B18 chronic viral hepatitis
B18.2 Chronic viral hepatitis with
Abbreviations used in the protocol
Ana - antinuclear antibodies
AMA - antimitochondrial antibodies
anti-HBC - HBCAG antibodies
anti-HBE - Hbeag antibodies
anti-HBS - antibodies to hbsag
anti-HCV - antibodies for hepatitis C virus
anti-HDV - antibodies for hepatitis D virus
anti-HIV - HIV antibodies
Hbeag - internal antigen of hepatitis virus in
HBSAG - hepatitis Virus Surface Antigen
HCV RNA - RNA HCV
IgG - immunoglobulins of class G.
IQR - interquartial coefficient
LBX - liver biopsy
Alt - alaninotransferase
ARVT - antiretroviral therapy
AST - aspartataminotransferase
AFP - alpha Fetoprotein
Achtv - activated partial thromboplastin time
Waart - high active antiretroviral therapy
VGA - viral Hepatitis A.
Vgv - viral Hepatitis B.
Vge - viral hepatitis E.
VGN - upper limit
HCV - viral hepatitis C.
HIV - aIDS virus
VN
VRV - varicose-extended veins
GGTP - gamma-GlutamylTranspendaz
ICC - hepatocellular carcinoma
D + ORD - combination of Dasabuvir with Obitasvir, Paritaprevir, Ritonavir
IL28B - Interleukin 28B
BMI - body mass index
IR - insulin resistance
IFA - linked immunosorbent assay
Iha - immunochemical analysis
CT - cT scan
INN - international non-proprietary title
Me - international Normalized Attitude
MRI - magnetic resonance imaging
Oak - general blood analysis
OAM - general urine analysis
OBR - abdominal organs
OGS - acute hepatitis C.
OST - opioid substitution therapy
PV - promrombin
PVT - antiviral therapy
Okifun - pegylated interferon
Pi - protombian index
PIN - consumers of injection nrokes
PCR - polymerase chain reaction
RBV - Ribavirin
RVO - early virological answer
RNA - ribonucleic acid
SD - Sugar Diabetes
SMV - Simeperevir
SE - erythrocyte sedimentation rate
AIDS - the syndrome of the acquired immunodeficiency
CVD cardiovascular diseases
TV - thromubic Time
TP - bien transplantation
Ttg - thyroid-stimulating hormone
Wois - sustainable virological answer
Ultrasound - ultrasound procedure
FPP - functional samples of the liver
Xg - chronic hepatitis
Hgs - chronic hepatitis C.
CPU - liver cirrhosis
SHF - alkaline phosphatase
EGDS - ezophagogastroduodenoscopy
ECG - electrocardiogram
Date of development of the Protocol: year 2014.
Date of revision of the protocol: 2015 year.
Protocol users:gastroenterologists, infectiousists, therapists, general practitioners, as well as doctors related specialties, carrying out maintenance and treatment of patients with hepatitis C at different stages of the disease.
Methodology:The protocol was developed on the basis of the clinical guidelines of leading international communities (WHO, EASL, AASLD, CASL, SASL, FASL, EACS, Ropype) and adapted to the methods of diagnosis and treatment used on the territory of Kazakhstan. The classification of the recommendations used in this protocol is presented in Table 1.
| BUT | High-quality meta-analysis, systematic overview of rock or large rock with a very low probability (++) systematic error |
| IN | High quality (++) systematic overview of cohort or studies Case-control or high-quality (++) cohort or studies Case control with a very low risk of systematic error or RCK with not high (+) risk of systematic error |
| FROM | Cohort or study case-control or controlled study without randomization with a low risk of systematic error (+) |
| D. | Description of a series of cases or uncontrolled research, or expert opinion |
Classification
Clinical classification:
The generally accepted classification of HSS does not exist.
When making a diagnosis, it is necessary to indicate the virological status (genotype and viral load), activity (biochemical and / or histological), as well as the stage of the disease (according to indirect elastography or morphological research)
Clinical picture
Cymptoms, flow
Diagnostic criteria:
The main criterion for the diagnosis of chronic hepatitis C is the presence of HCV RNA over 6 months.
Complaints and history:
Chronic hepatitis C proceeds asymptomatic or low-minded and can be accompanied by such non-specific symptoms as:
· Fatigue;
· Influense symptoms;
· joint pain;
· Itching;
· Sleep impairment and appetite;
· Nausea;
· Depression (evaluated in all patients using the Beck scale).
Chronic hepatitis C can be associated with extrahepatic manifestations, such as:
· Depression (evaluated in all patients using the Beka scale);
· Cryoglobulinemia;
· B-cell lymphoproliferative diseases;
· Late skin porphyria;
· Vasculitis;
· Red flat deprived;
· Shegren syndrome;
· Glomerulonephritis;
· Type sugar diabetes.
When collecting anamnesis, instructions on hemotransphus, organs and tissue transplantation, unsafe invasive (non-medical) manipulations, belonging to risk groups (drug users, faces with random sexual bonds, patients on chronic hemodialysis, patients with oncohematological diseases, persons living With HIV and other parenteral infections, sexual partners of individuals with HCV, medical workers, children born from HCV-infected mothers, faces with changed functional liver tests). Persons with these risk factors require preventive screening for HCV (ANTI-HCV)
Physical examination:
In a physical examination at the initial stage of the HSS, pathology is not detected, with the exception of minor hepatomegaly. As the disease progresses, the increase and sealing of the liver may be occurred. Splenomegaly and other stigmas chronic liver disease can manifest itself at later stages.
Viral hepatitis with predominantly proceeds asymptomatic. In the transition of chronic hepatitis C in cirrhosis in 6.4% of cases, symptoms were noted due to dysfunction of the liver and portal hypertension:
· Peripheral swelling;
· Ascites;
· Jaundice;
· Blooding and bleeding;
· Star hemangiomas (teleangioectasis);
· Hair loss on the skin of the chest and abdomen (in men);
· Gynecomastia;
· Varicose veins of the esophagus and stomach;
· Disruption of cognitive functions associated with hepatic encephalopathy.
In some cases, HCS is detected in patients with the GCC, which, as a rule, proceeds asymptomatic, except the incidents of the running stage, when the tumor reaches a significant size, causing deterioration of the liver function (jaundice, ascites, hepatic encephalopathy), pain in the upper right quadrant, asthenization and Weight loss.
Diagnostics
List of basic and additional diagnostic events
Main (mandatory) diagnostic surveys conducted on an outpatient level: Specified in Table 2.
Additional diagnostic surveys conducted on an outpatient level:specified in Table 2.
The minimum list of the survey, which must be carried out in the direction of the planned hospitalization: according to the internal regulation of the hospital, taking into account the current order of the authorized body in the field of health.
Main (mandatory) diagnostic surveys conducted at the stationary level correspond to those on the outpatient level and are presented in Table 2.
Additional diagnostic surveys conducted at the stationary level, correspond to those on the outpatient level and are presented in Table 2. 
Instrumental research
Radiological research
Radiological liver study (first of all ultrasound) allows you to identify the signs of steatosis, pronounced fibrosis and transition to liver cirrhosis (rounding of liver contours, uneven surfaces and coarse-grained liver parenchyma), signs of portal hypertension and thrombosis (increase in diameter, cavernous transformation, spleen veins, ascites, splenomegaly), as well as the presence of volume formations (ICC). Other visualizing technologies (CT, MRI) can be used.
Endoscopic study
Allows you to identify such signs of portal hypertension as varicose veins (esophagus and stomach) and portal gastroptoam in patients with liver cirrhosis in the outcome of the HSS.
Study of the stage of fibrosis
Estimation of the severity of the liver disease should be carried out before PVT. The identification of patients with cirrhosis of the liver is of particular importance, since the efficiency of PVT is inversely proportional to the fibrosis stage. The lack of pronounced fibrosis matters when deciding on the time of the beginning of PVT. Patients with obvious clinical signs of cirrhosis do not need liver biopsy to assess the fibrosis stage. Patients with signs of liver cirrhosis must be examined on the ICC. The pronounced fibrosis can be in patients with the normal activity of Alt, so the assessment of the degree of gravity of the disease should be carried out regardless of the indicators of Alt. The puncture biopsy remains a reference method of assessing the liver fibrosis stage. The risk of severe complications for biopsy is very low (from 1/4000 to 1/10000). In patients with violation of blood clotting, a trans-car biopsy liver with a simultaneous pressure estimate in the portal vein can be used.
With HGS alternative, non-invasive methods (indirect elastography and biomarkers) can be used instead of biopsy.
Indirect elastography can be used to estimate the liver fibrosis stage in patients with HSS, but it is necessary to take into account the factors that may affect the accuracy of the results, for example, the pronounced activity of the disease, obesity.
Both methods (indirect elastography and biomarkers) are accurate when evaluating cirrhosis and zero fibrosis, but less accurate at intermediate fibrosis stages. The combination of biomarkers and indirect elastography increases the accuracy of the assessment of the fibrosis stage and reduces the need for a puncture biopsy. In the case of contradictory results of biomarkers and indirect elastography, you can use the lining biopsy of the liver. Histological assessment is also necessary in mixed etiology (for example, HCV with VGV, metabolic syndrome, alcoholism or autoimmune diseases)
Penal biopsy liver (PBP) - relatively safe method for assessing morphological changes in liver in patients with HGS. PBP allows us to evaluate the severity of the fibrotic process and non-exposure changes. The PBP results are easily interpreted and amenable to a semi-quantitative assessment. The PBP is carried out in the dynamics in order to assess the progression of liver damage at HGS. PBP is the only available method that allows to assess the contribution of concomitant diseases (steatohematitis, hemochromatosis, autoimmune hepatitis, etc.) in the pathological process and their effect on the course and effectiveness of the treatment of HSS. It must be remembered that the PBP has a number of restrictions. In particular, the experience of a doctor conducting puncture, and a morphologist, evaluating morphological changes, is important; Small volume of liver tissue samples; invasiveness and discomfort for patients; The risk of developing complications. PBP requires strict execution of rules for its implementation in the conditions of specialized departments and the presence of qualified morphologists. The rules for conducting a puncture biopsy of the liver are presented in Appendix 1, and the interpretation of the results is in tables 4 and 5.
Table 4. Morphological diagnostics of the degree of non-political activity of hepatitis
| Histological diagnosis | Metavir. | Knodell (IV) | Ishak. |
| Xg minimal activity | A1. | 0-3 | 0-3 |
| Xg of low-rise activity | A1. | 4-5 | 4-6 |
| Xg moderate activity | A2. | 6-9 | 7-9 |
| Xg of pronounced activity | A3. | 10-12 | 10-15 |
| Xg of pronounced activity with bridge necrosis | A3. | 13-18 | 16-18 |
Table 5. Morphological diagnosis of the stage of the liver disease (fibrosis severity)
| Stage Fibrosis | Metavir.* | Knodell (IV) | Ishak. |
| No fibrosis | F0. | 0 | 0 |
| Portal fibrosis of several portal paths | F1 | 1 | 1 |
| Portal fibrosis of most portal tracts | F1 | 1 | 2 |
| Several bridge fibrous sept | F2. | 3 | 3 |
| Many bridge fibrous sept | F3. | 3 | 4 |
| Incomplete cirrhosis | F4. | 4 | 5 |
| Fully formed cirrhosis | F4. | 4 | 6 |
* To determine the stage of the liver disease, the Metavir scale is more often applied.
Measurement of liver elasticity (indirect elastography or elastometry)it is carried out on the FIBROSCAN apparatus and allows you to judge the change in the elastic properties of the liver based on the reflected vibration pulses and the subsequent computer analysis. The interpretation of the results of indirect elastography is presented in Table 6.
The benefits of the method include:
· Non-invasiveness
· Reproducibility
· Larger than during biopsy evaluated liver tissue (100-200 times more)
· The speed and ease of use (the survey occupies an average of 5 minutes)
· Immediate result
· Evaluation of the effectiveness of therapy
· Children's ability to examine
Interpretation of the results of elastometry is difficult in cases:
· Excess weight (BMI\u003e 35 kg / m 2)
· Pronounced liver steatosis
· High biochemical activity (Alt / AST above the upper limit of the norm in 3 or more times)
· Pronounced cholestasis
· Constant heart failure
Criteria of the successful result of the study:
· Intercom coefficient (IQR) - no more than 30% of the elasticity indicator
· At least 10 reliable measurements at one study point
· At least 60% of successful measurements
Under the excess mass of the body, the extension of elastometry with the use of the XL sensor is advisable to be expediently with fat hepatosis.
Table 6. Interpretation of the results of indirect elastography
|
Histological data |
The results of the indirect liver elastometry on the FIBROScan apparatus | |
|
Stage Metavir fibrosis |
Scope Values, kpa |
Diagnostic Accuracy,% |
| F0. | 1,5 - 5,8 | 88,6 |
| F1 | 5,9 - 7,2 | 87,2 |
| F2. | 7,3 - 9,5 | 93,2 |
| F3. | 9,6 - 12,4 | 90,9 |
| F4. | More than 12.4. | 95,5 |
Biomarkersdefined using laboratory tests and allow us to evaluate the activity of the non-exposure process (Actitest and the analogs) and the severity of liver fibrosis (fibrotest and analogs). Interpretation of the results of biomarket tests is shown in Tables 7 and 8.
Table 7. Interpretation of Actitest results
| Degree of non-political activity on Metavir | Actitest results |
| A0. | 0,00 - 0,17 |
| A0 - A1. | 0,18 - 0,29 |
| A1. | 0,30 - 0,36 |
| A1 - A2. | 0,37 - 0,52 |
| A2. | 0,53 - 0,60 |
| A2 - A3. | 0,61 - 0,62 |
| A3. | 0,63 - 1,00 |
Table 8. Interpretation of FIBROTEST results
| FIBROTEST results | Metavir. | Knodell. | Ishak. |
| 0,00 - 0,21 | F0. | F0. | F0. |
| 0,22 - 0,27 | F0-F1 | F0-F1 | F1 |
| 0,28 - 0,31 | F1 | F1 | F2. |
| 0,32 - 0,48 | F1-2 | F1-F3. | F2-3. |
| 0,49 - 0,58 | F2. | F1-F3. | F3. |
| 0,59 - 0,72 | F3. | F3. | F4. |
| 0,73 - 0,74 | F3-4 | F3-F4. | F5. |
| 0,75 - 1,00 | F4. | F4. | F6. |
· Consultation of the ophthalmologist (the state of the eye dna) - before and during PVT;
· Consultation of the psychiatrist - with suspicion of depression;
· Consultation of a dermatologist / allergologist / rheumatologist - in the presence of skin / allergic and autoimmune reactions;
· Consultation of the oncologist - with suspected of the ICC;
· Consultation of other specialists - on clinical indications.
Laboratory diagnostics
Laboratory research:
Studies necessary for all patients with HCV:
OAK with thrombocyte count. Anemia (as a result of hyperslenism, bleeding from VRV), leukopenia, thrombocytopenia (as a result of hypersplenism and direct myelodepressive effects of HCV) can be detected, the acceleration of ESO (with infectious complications).
Biochemical profile includes identifying indicators of ALT, AST, GGTP, albumin, bilirubin, alkaline phosphatase, many or PV, as well as routine (glucose, creatinine, cholesterol) and some specific indicators, such as gamma globulines, IgG (autoimmune hepatitis screening), serum Iron and ferritin (hemochromatosis screening and secondary irradiation with iron), cerulinsmine (screening of Wilson-Konovalov's disease), AFP (Scronging of the CCC). The activity of Alt and Ast may be minimal (< ВГН), слабовыраженной (< 5 ВГН), умеренной (5-10 ВГН), выраженной (> 10 VGN) and does not always correlate with histological activity. Bilirubin level with HSS, as a rule, normal. Its increase can be observed in acute hepatitis or indicate a worsening of the liver activity at the late stage of the disease, which is also accompanied by a decrease in the level of albumin and an increase in MNO or PV. Indicators of alkaline phosphatase and GGTP may increase with acute hepatitis and remain at the level of the norm during chronic hepatitis.
The clinical laboratory survey plan also includes OAM, coprogram.
Serological Studies (IHA / IFA)includes Anti-HCV definition, other parenteral infections such as HBSAG, HBEAG, Anti-HBS, Anti-HBE, Anti-HBC Total / IgM), AT (Anti-HDV with HBSAG carriers), HIV (ANTI-HIV) , as well as (with suspicion of acute hepatitis) VGA (Anti-HAV) and VGU (anti-hev)
Molecular diagnosisincludes a qualitative definition of HCV RNA using highly sensitive PCR in real time with a lower limit of 15 me / ml definition on automatic closed type analyzers. In general, virological diagnosis is carried out on the basis of the following principles:
· Definition of Anti-HCV is the first diagnostic line of HCV (Recommendation A1);
· In the case of suspicion of acute HCV or immunosuppressive patients, it is necessary to determine the HCV RNA (Recommendation A1);
· If an anti-hcv test is positive, it is necessary to define HCV RNA, a sensitive molecular method (Recommendation A1);
· Patients with a positive Anti-HCV test and a negative molecular test on HCV RNA must be tested on HCV RNA after 3 months to confirm the elimination of the virus (Recommendation A1).
The interpretation of the results of IH / IFA and PCR is carried out according to Table 3.
Table 3. Interpretation of the results of IHA / ELISA and PCR
| Markers | Interpretation | Further tactic |
|
anti-HCV (+) HCV RNA (+) |
· HCV |
Establishing the activity and stage of the disease, when determining the testimony to the PVT - a quantitative test of PCR and genotyping |
|
anti-HCV (-) HCV RNA (+) |
· Laboratory error · OGS (in the first weeks) - ELFA (+) 50% at the moment of acute manifestations, so PCR, with suspected OGS, is carried out in all, including IFA (-) cases · HCV in people with immunosuppression - Patients receiving immunosuppressive drugs - are hemodialysis - After transplantation - Patients with HIV infection |
ELISA and PCR in dynamics |
|
anti-HCV (+) HCV RNA (-) |
- recovered patients after the suffered hepatitis C (shelterfection) - false positive result of the IFA - passively acquired antibodies during hemotransfusion - Passively acquired mother antibodies - Intermitting Viryiai |
PCR in 3 months to confirm the elimination of the virus |
Studies conducted in patients before planned PVT
Molecular diagnosisincludes: Quantitative Definition of HCV RNA using highly sensitive PCR in real time with a lower limit of 15 me / ml definition on an automatic closed type analyzer, as well as the definition of GSS genotype.
Currently known 6 different types Virus, which are denoted by numbers from 1 to 6. There are also subtypes indicated by letters (for example, subtype 1a and 1b). In the territory of the Republic of Kazakhstan, 1b, 2 and 3 genotypes are predominantly distributed.
Functional Samples of the Thyroid gland (TTG)
Pregnancy test
Determination of polymorphism of the interleukin-28B gene.The result of the analysis of polymorphism in the IL28B gene is useful in the forecast of the effectiveness of the treatment and decision on the choice of regime of therapy in patients with HCV 1 genotype.
In recent years, the feasibility of the study of the polymorphism of the IL28B gene as a predictor of the achievement of uvo, both in the case of dual therapy of Penggent and during triple therapy with the inclusion of protease inhibitors in patients with genotype 1 HCV. The IL28B gene encoding the interferon of the 3rd type lambda is located on the 19th chromosome. A high predictive value regarding the achievement of WEVO has a single-flowered polymorphism of alleles C (cytosine) or T (Timin) at the RS12979860 position. The SS genotype is approximately 2 times more common in patients with spontaneous GSS clearance in acute hepatitis C in comparison with those whose infection has acquired a chronic course. Among the PCS patients with a genotype of 1 of the Europeanid race, treated peginf and having SS genotypes, ST and TT, a steady virological response is achieved by 69%, 33% and 27%, respectively. The predictive value of the determination of the polymorphism of the IL28B gene relative to the achievement of UVV at the PVT planning stage is higher than the predictive strength of the level of viral load, the stage of fibrosis, age and the patient floor.
Differential diagnosis
Differential diagnosis:
It is carried out with other hepatitis (Table 9)
Table 9. Differential diagnosis of HGS
| Name of nosology | Features |
| Viral hepatitis B. | Availability of HBSAG, HBV DNA serum |
| Viral hepatitis D. | Availability Anti-HDV (Total, Igm), HDV RNA in blood serum |
| Non alcoholic steatohepatitis | Detection of fatty infiltration for morphological or one of the visualizing studies (ultrasound, CT, MRI) in patients who do not consume toxic doses (less than 20 g of ethanol per day for women and less than 30 g of ethanol per day for men), the presence of components of metabolic syndrome (Dyslipidemia, SD, AG, Obesity) |
| Alcoholic liver disease | Alcoholic history (drinking alcohol in toxic doses, positive results of Cage and Audit questionnaires), alcoholic "stigma" - hyperemia of the wings of the nose, an increase in the parish glands, contracture of dupiet, macrocytosis, the value of the de ritis coefficient (AST / Alt) is greater than 2 in the absence of severe fibrosis / CPU, raising GGT with normal alkaline phosphatase activity, an increase in IGA concentration in serum |
| Vilson-Konovalov disease | The age of patients under 45 years of age, the presence of a kaiser-flasher ring, a decrease in serum ceruloplasmin, an increase in the daily excretion of copper with urine, mutation in the APR3V gene |
| Autimmune hepatitis | Diagnostic titers of autoantibodies, an increase in IgG, hyper-gammaglobulinemia, characteristic histological changes (border hepatitis, lymphoplasmatic infiltration) |
| Primary biliary cholangitis (cirrhosis) | The presence of clinical and biochemical cholestasis syndrome, the presence of antimitochondrial antibodies, an increase in IgM, characteristic histological changes (non-resident destructive cholangitis) |
| Primary sclerosing cholangitis | The presence of clinical and biochemical cholestasis syndrome, detection of deformation and strictures of bile ducts with MP and endoscopic retrograde cholangiography, characteristic histological changes (bile duct fibroids) |
| Alfa-1-AntitripSin insufficiency | Reducing the level of alpha globulin in the electrophoresis of serum proteins, serum alpha-1-antitripxin, mutations in the A1T gene |
| Hereditary hemochromatosis | Improving the level of iron serum, ferritin, reduction of the yazss, mutations in the HFE gene |
| Medicinal lesion of the liver | Reception of hepatotoxic drugs in history in previous 6 months, the presence of concomitant diseases requiring constant therapy |
Treatment abroad
Treat treatment in Korea, Israel, Germany, USA
Get advice on medical examination
Treatment
Treats of treatment
· Eradication of HCV in order to prevent the development of the liver cirrhosis, FCC and death (Recommendation A1)
· In patients with cirrhosis of the liver - decrease in the frequency of decompensation and risk of the ICC (for this group of patients, it is necessary to continue screening of the CCC) (Recommendation A1)
· The end point of therapy is a steady virological response (WEV) - an indefinable level of HCV RNA (<15 МЕ/мл) на 24 неделе после окончания терапии (рекомендация A1)
Tactics of treatment:
Non-drug treatment:
· Security regime (avoid insolation, overheating of the body, in advanced stages of disease and portal hypertension - restriction of physical exertion, facilitating the mode of operation)
· Abundant drink up to 2-3 liters per day
· Minimization of progression risk factors (elimination of alcohol, tobacco, marijuana, hepatotoxic medicines, including biologically active additives, normalization of body weight, etc.)
Medical treatment:
The basis of the treatment of HSS is PVT based on a combination of pegylated interferon, ribavirin, as well as direct antiviral agents. The list of basic medicines approved for the treatment of HSS in the Republic of Kazakhstan is presented in Table 10. After approval in the RK of other antiviral drugs, they should be applied in accordance with the officially approved instructions.
Table 10. List of medicines approved for the treatment of HSS in the Republic of Kazakhstan
| MNN |
Pharmacotherapeutic Group |
Form release |
|
Interferons. PBX code L03Av11 |
Injection 180 μg / 0.5 ml |
|
|
Pegylated Interferon alpha-2b |
Interferons. PBX code L03AB10 |
Injection 50 μg / 0.5 ml 80 μg / 0.5 ml 100 μg / 0.5 ml 120 μg / 0.5 ml 150 μg / 0.5 ml |
| Ribavirin |
PBX code J05AB04 |
Capsules / Tablets 200 mg |
| SimePrevir |
Code ATC J05AE14. |
Capsules 150 mg |
|
Code ATX J05A. |
Tablets set containing: Dasabuvir 250 mg; Ombitasvir 12.5 mg + parityarerevir 75 mg + ritonavir 50 mg |
Indications to start PVT:
· All patients with HCS with compensated liver disease should be considered as candidates for the assignment of therapy (Recommendation A1)
· Treatment of patients with F3-F4 fibrosis stages on Metavir should be held primarily (recommendation A1)
· Treatment of patients with F2 F2 on Metavir fibrosis is shown in a planned manner, while the priority in obtaining therapy should have patients with the following diseases / relating to the following categories:
- organ transplantation (recommendation B1)
- extrahepatic manifestations, such as essential mixed cryoglobulinemia 2 or 3 types with lesion of remote organs (vasculitis, etc.), late skin porphyria (recommendation B1)
- Coinfection HIV-1 (recommendation B1)
- HBV coinfection (Recommendation C2)
- SD 2 types and IR (recommendation B2)
- Patients on chronic hemodialysis (Recommendation C2)
- HCV-infected women planning pregnancy (C1 recommendation)
· Patients with less severe disease (F0-F1) Conducting therapy may be considered individually (recommendation B1).
Contraindications to start PVT based on interferon
Absolute contraindications:
· Uncontrollable depression
· Psychosis
· Epilepsy (if it is impossible to ensure the control of the disease)
· Uncontrolled autoimmune diseases
· Children's age up to 18 years old (for triple therapy)
· Pregnancy and reluctance of compliance with contraception
· Heavy concomitant diseases
- Heart failure
- poorly controlled SD
- poorly controlled arterial hypertension
- chronic obstructive pulmonary disease (COPD)
Relative contraindications:
· Hematological changes
· HB.<130 г/л (муж), 120 г/л (жен)
· Neutrophils<1500/мл
· Thrombocytes<90,000/мл
· Creatine\u003e 1.5 mg / dL (132.6 μmol / l)
· Decompensated CPU
· Other specified in the instructions for the use of drugs
Contraindications for the start of PVT based on D + ORD
· Decompensated liver cirrhosis (class in child-drink and above), including in history
· Children's age up to 18 years
· Failure contraception, pregnancy, breastfeeding
· Lactase deficiency, galactose intolerance, glucose-galactose malabsorption
· Allergic reactions to rhythonavir history
· Contraindications for destination Ribavirin (when combined with it)
Monitoring a virological response
During PVT, fast virological response (BVO) is estimated, early virological response (RVO, which can be complete and incomplete), full of slow virological response (MVO), direct response or response to the end of therapy (OOT), steady virological response (WEV) , zero response, partial answer, virological breakthrough and relapse according to the criteria presented in Table 11.
Table 11. Monitoring antiviral therapy based on interferon. Options for response to treatment
| Combination / answer | Definition |
| FeGIFN / RBV | |
| Fast virological response (BVO) | The undefined level of HCV RNA in the blood for the 4th week of treatment |
| Early Virological Answer (RVO) \u003d \u200b\u200bEarly Full Virological Response | The undefined level of HCV RNA in the blood for the 12th week of treatment, preserving until the end of treatment |
| Slow virology answer (MVO) \u003d \u200b\u200bEarly incomplete virological response | The reduction in the level of HCV RNA in the blood is more than 2 log10 below the initial on the 12th week of therapy, but the undefined level is not achieved. On 24 weeks of treatment, the HCV RNA level is no longer determined and persisted indefinitely until the end of treatment |
| Reply at the end of therapy (OOT) | Undermined HCV RNA level at the end of therapy |
| Sustainable virus response (WEV) | The undefined level of HCV RNA in the blood 24 weeks after the end of treatment |
| Zero answer | Reduced HCV RNA level in blood less than 2 log10 on the 12th week of treatment |
| Partial answer | Reducing the HCV RNA level in the blood of more than 2 log10 on the 12th week of therapy, but at the same time the undefined level of HCV RNA is not achieved both at 12 and on the 24th week of treatment |
| Virological breakthrough |
Re-appearance HCV RNA in blood After reaching the undefined level of HCV RNA at any time in the process of antiviral therapy |
| Recurd | The appearance of HCV RNA in the blood for 24 weeks after the end of a successful course of therapy (i.e., after reaching the undue HCV RNA level at the end of the treatment) |
General recommendations for the conduct of PVT
· Complete commitment to PVT - an important factor in achieving IVV (Recommendation A1)
· Both PEGIFN-α2A molecules (180 μg / week) and PAGIFN-α2B (1.5 μg / kg / week) can be used in double and triple therapy (recommendation B1)
· Overweight negatively affects the achievement of WSV (Recommendation A2). Reducing weight when it is redundant before PVT can increase the likelihood of achieving IVV (Recommendation C2)
· Insulin resistance is associated with the failure of PVT, but at the moment there is no sufficient evidence base of using insulinsintyasers in this category of patients (C2 recommendation)
· Patients are recommended to abstain from alcohol use during PVT (C1 recommendation)
· Permanent supporting therapy using low doses Permanent NEGIFN is not recommended (Recommendation A1)
· To monitor the effectiveness of PVT, use PCR analysis in real time with the lower limit of the definition<15 МЕ/мл на анализаторах закрытого типа (рекомендация B1)
· In order to assess the effectiveness of PVT, the virological response is determined during therapy (after 4 weeks), at the end of therapy, as well as 24 weeks after the end of treatment (WEV) (A2 Recommendation)
· The threshold level for the difference between the low V HV from high, is the HCV RNA level 400,000 me / ml (Recommendation C2)
· Before starting PVT, it is necessary to evaluate all possible drug interactions. Due to the fact that a list of drugs with possible interactions is constantly updated, it is necessary first to contact the instructions for medical use of the drug, and use accessible on-line resources (for example, www.hep-druginteractions.org)
· During therapy and the first 6 months after its end, it is necessary to comply with the effective (double) contraception.
Recommendations for PVT in patients with HGS caused by a virus 1 genotype
· In patients with HGS caused by a genotype virus 1, double therapy schemes, triple therapy based on interferon, as well as without interferonic therapy with direct antiviral agents can be used
· In patients with HGS, caused by a virus 1 of the genotype, previously not received by PVT, with the stage of the disease, previously not received PVTs, with a high probability of achieving WEVO (with a disease stage · in patients with HGS, caused by a virus 1 of the genotype, with the failure of the preceding Double therapy, re-treatment should be carried out in the mode of triple therapy or without interferon therapy with direct antiviral agents (recommendation A1).
· In patients with HGS, caused by a virus 1 of the genotype, with contraindications to interferon, treatment should be carried out in non-interferonic therapy mode with direct antiviral agents (Recommendation A1)
· In all other cases, patients with HGS, caused by a virus 1 of the genotype, previously not received by PVT, the choice in favor of double, triple therapy based on interferon or without interferon therapy is determined individually
Recommendations for dual PVT in patients with HGS caused by viruses 1 and 4 genotypes
· With double therapy, the Dose RBV must be selected based on the patient's weight, 15 mg / kg (recommendation B2).
· The duration of therapy is determined by the initial characteristics of the patient, the virus, as well as the virological response to 4, 12, (24) weakens of treatment. The probability of WSV is directly proportional to the HCV RNA clearance speed (recommendation B1).
· In patients who have reached the BVA, with the initial high VN (\u003e 400,000 me / ml) and / or having adverse factors, as well as in patients who have reached the RFA (without a BVA), the recommended duration of therapy is 48 weeks.
· In patients with source low VN (<400,000 МЕ/мл), отсутствием неблагоприятных факторов и достигших БВО при лечении в режиме двойной терапии, можно рассмотреть вариант сокращения длительности лечения до 24 недель.
· In patients who have reached the MVO, the optimal duration of treatment should be 72 weeks (recommendation B2).
· Therapy should be stopped for 12 week, if by this time the HCV RNA level decreased by less than 2 log10 me / ml or if HCV RNA is determined on the 24th week of treatment (Recommendation B1).
· Algorithm of treatment in dual-therapy CGS mode caused by a virus 1 of the genotype is shown in the Scheme 1 of Annex 2.
Triple PVT recommendations in patients with HGS caused by the 1 genotype virus
· In the schemes of triple therapy in combination with Peginf and RBV, the second generation protease inhibitor is used - SimePrevir (SMV) (Recommendation A1).
· The use of first-generation protease inhibitors (teleprevir and boozerevir) is not recommended.
· With triple therapy, the dose of RBV must be defined according to the instructions. The dose of protease inhibitor cannot be reduced, and in case of cancellation of the drug, its reception can not be resumed.
· Patients with the failure of PVT, which have not been specified by the version of the virological response (relapse, partial response, zero response, virological breakthrough), should not receive a shortened re-PVT course.
· Patients with the failure of triple therapy using a protease inhibitor should not receive a re-course by a similar scheme.
· Basic principles of triple therapy with SimePrevir (SMV):
- The recommended dose of SMV is 150 mg per day and is accepted in 1 reception along with food
- If the delay in the operation of the SMV was less than 12 hours, then the missed dose should be taken as early as possible and further resume the normal dosing mode. If late in reception of the SimePrevir was more than 12 hours, then the missed dose should not be taken, and the next dose is accepted into the usual time on schedule
- in patients regardless of the availability of CPU previously not received treatment, as well as recurrent patients, the total duration of therapy is 24 weeks and consists of a 12-week course of triple therapy and the subsequent 12-week courses of double therapy (Recommendation A1)
- in patients with CPU and co-infection of HIV previously received treatment or preceding recurrence, the total duration of therapy is 48 weeks and consists of a 12-week course of triple therapy and the subsequent 36-week courses of double therapy (A1 recommendation)
- in patients regardless of the availability of CPU, with a preceding partial or zero response, the total duration of therapy is 48 weeks and consists of a 12-week course of triple therapy and the subsequent 36-week of double therapy (Recommendation A1)
- During triple therapy with Simeperevir, the definition of HCV RNA should be carried out by 4, 12 and 24 weeks and at the time of the end of treatment (Recommendation A2)
- Triple therapy with Simeperevir must be stopped if the HCV RNA level ≥ 25 IU / ml per 4 or 12 or 24 weeks of treatment (Recommendation A1)
- In the Republic of Kazakhstan 1 Genotype of the hepatitis virus with virtually all patients is represented by the subtype of "B" (Gogotype 1B HCV). In case of detection of the HCV genotype 1A, before starting treatment, it is necessary to conduct a study for the presence of NS3 Q80K polymorphism of the virus and, in case of detection of this polymorphism, carrying out triple therapy based on Peginf-α, RBV and SMV inexpediently due to its predicted inefficiency
- Algorithm for the treatment of HSS caused by a virus 1 of the genotype using triple therapy with the SMV is presented in the Scheme 2 of Annex 2.
Recommendations for non-interferon therapy with direct antiviral agents in patients with HGS caused by a virus 1 genotype
. In non-interferonic therapy mode, a combination of dasabuvir with Ombitasvir, parityarevir, ritonavir (D + ORD) is used.
· The recommended dose of d + ODA includes one dasabuvir tablet 250 mg twice a day (in the morning and evening) and two Obitasvira / Paritaprevir / Ritonavir 12.5 / 75/50 mg pills once a day (in the morning). In patients with liver cirrhosis, as well as in all patients, infected with the genotype 1A virus, D + ODA is used in combination with RBV
. For patients with HGS, caused by a virus 1a of the genotype, without cirrhosis, first beginner treatment or after the failure of the IFN and RBV therapy fails, the duration of therapy is 12 weeks
. For patients with HGS, caused by a virus 1a of the genotype with compensated cirrhosis, the duration of therapy is 24 weeks
. For patients with HGS, caused by the 1B genotype virus, first novice treatment or after the failure of the IFN and RBV therapy, without cirrhosis or compensated cirrhosis, the duration of therapy is 12 weeks
. When using RBV, its dose must be defined according to the instructions.
. The HGS treatment algorithm caused by a genotype virus using non-interferon mode based on D + ODA is shown in the Scheme 3 of Annex 2.
Recommendations for PVT in patients with HGS caused by viruses 2.3 (5.6) genotypes
· In patients with HGS, caused by viruses of 2.3 genotypes, a pattern of therapy based on the combination of Patterns and RBV
· In patients with HGS caused by viruses 2 and 3 genotypes, the dose of RBV should be 800 mg / day (Recommendation A2). In the presence of adverse factors (BMI\u003e 25, IR, MS, heavy fibrosis, CPU or senior age) Dose RBV should be seized based on the calculation of 15mg / kg
· Patients with HGS caused by viruses 5 and 6 genotypes, Dose RBV should be 15mg / kg (recommendation A2)
· High or low source viral load may be a useful criterion for the treatment of dual therapy patients (recommendation B2).
· The duration of therapy is determined by the initial characteristics of the patient, the virus, as well as the virological response to 4, 12, (24) weakens of treatment. The probability of IVV is directly proportional to the HCV RNA clearance speed (recommendation B1)
· In patients who have reached the BVO who do not have adverse factors, the duration of therapy is 24 weeks
· In patients who have reached the PBQ (without BVA), the duration of therapy is 24 weeks. It is possible to consider increasing the length of therapy in this category of patients up to 48 weeks, especially in the presence of adverse factors, in order to increase the likelihood of achieving IVV
· In patients who have reached MVO, the duration of therapy should be 48 weeks
· Therapy should be stopped for 12 weeks if by this time the HCV RNA level decreased by less than 2 log10 me / ml or if HCV RNA is determined on the 24th week of treatment (Recommendation B1)
· Patients with the failure of previous therapy subject to the presence of readings may be appointed by the PVT-based PVT based on PVT and RBV until other treatment options are available (Recommendation B2)
· Algorithm for the treatment of HSS, caused by viruses of 2.3 genotypes, in double therapy mode is shown in Scheme 3 of Annex 2.
Correction of side effects of PVT
The correction of the most frequent side effects should be carried out according to Table 12
Table 12. Correction of the most frequent side phenomena of PVT (Recommendation C2)
| Sociality | Tactics |
| Influense Symptoms, Malgy, Arthralgia |
· Paracetamol (0.5-1 g 30 minutes to IFN) · Splashing mode · Drink (2-3 liters per day) |
| Lesion of the skin at the injection site |
· Check technology · Injection to another area |
| Heavy controlled depression |
Reducing the dose of the PEGIFN-α 2A \u200b\u200baccording to the scheme: 180mg / week → 135mg / week → 90mg / week Reducing the dose of Peregypn-α 2B according to the scheme: 1,5mg / kg / week → 1mg / kg / week → 0,5mg / kg / week Or the use of altarrombopag thrombopoeatetine agonist (25-25 mg / day) until the target target level is reached |
|
Absolute number of neutrophils < 750/мм³ |
|
| Thrombocytes< 50,000/мм³ | |
| Hemoglobin<100 г/л | Reduced dose of RBV for 200mg (minimum dose 400 mg / day) |
| Heavy uncontrollable depression |
Cancellation of Ognifn-α 2A \u200b\u200b/ 2B If the number of neutrophils and platelets began to increase, it is possible to resume the injection of the perch, but with a reduced dosage The use of the thrombopoeatetin elcropag agonist (25-50 mg / day) until the target level is reached |
|
Absolute number of neutrophils < 500/мм³ |
|
| Thrombocytes< 25,000/мм³ | |
| Hemoglobin<8 5г/л | Cancel RBV |
| The increase in Alt is 10 times higher than the norm (if this was not at the time of the start of therapy) | Cancel all therapy |
| Heavy bacterial infection / sepsis (regardless of the number of neutrophils) | |
| Thyroid dysfunction |
· Correction of hypothyroidism and hyperthyroidism according to the relevant protocols · With clinically pronounced hyperthyroidism - termination of PVT |
| The aggravation of autoimmune diseases | Cancel all therapy |
| Improving the level of bilirubin in the blood without increasing the level of liver transamamine on the background of triple therapy with SimePrevir | Changing therapy mode is not required |
| Reactions photosensitivity | During treatment with Simeperevir, it is necessary to avoid excessive insolation and the use of apparatus for artificial tanning |
| Rash | When developing severe rash - the abolition of all therapy |
· To avoid cancellation of the runifun or RBV, in case the reduction in doses does not improve the hemogram, the use of growth factors is possible (Recommendation C2)
· Recombinant erythropoietin can be used by reducing Hb levels below 100 g / l, in order to avoid a reduction in the dose or cancellation of the RBV, especially in patients with CPU (C2 Recommendation)
· Thrombopoietin agonist can be used in order to correct the thrombocytopenia to avoid dose reduction or cancellation, especially in patients with CPU (C2 Recommendation); At the same time, it is necessary to keep due to the risk of development of thrombotic complications (in individuals with CPU and with a reduced level of albumin<35 г/л и возрасте старше 60 лет)
· There are no sufficient evidence that neutropenia during PVT is associated with a greater frequency of development of infectious complications, as well as the use of a granulocytic colonystimulating factor reduces the frequency of infections and / or increases the likelihood of achieving IVV (recommendation B1)
· Patients with signs or history of depression should be examined by a psychiatrist before the start of PVT. Patients with depression, which respected during PVT, shows the appointment of antidepressants. Preventive antidepressant therapy in some cases can reduce the frequency of development of depression, without affecting the achievement of IVV (recommendation B2)
Patients with compensated cirrhosis
Treatment is highly recommended for patients with compensated cirrhosis to prevent complications of HGS, which occur in this group of patients in the short-term and medium term. Large cohort studies and meta-analyzes have shown that the achievement of WSV in patients with severe fibrosis is associated with a significant decrease in cases of decompensation and development of the ICC.
· In the absence of contraindications, patients with compensated cirrhosis of the liver should receive treatment to prevent the development of short-term and long-term complications (recommendation B2)
· Monitoring and management of side effects, especially in patients with portal hypertension, low platelet (<100,000/мл), лейкоцитов, эритроцитов и низким уровнем альбумина в плазме (35г/л) должен быть особенно тщательным. Факторы роста (рекомбинантный эритропоэтин, агонист тромбопоэтина) могут быть полезны для данной группы пациентов, находящихся на интерферонотерапии (рекомендация C2)
· Regardless of the presence of WEV, patients with liver cirrhosis, it is necessary to carry out ultrasound over 3-6 months and determine the level of AFP in order to screening the FCC, (Recommendation A1)
Patients who show liver transplantation
Liver transplantation is a method for choosing for patients with terminal staging of liver disease. However, with HCV, the graft is re-infected after transplantation.
· In patients waiting for the liver transplantation, PVT when achieving IVV prevents possible re-infection of the graft (recommendation B2)
· PVT can be started during the expectation of TP in order to achieve an IVV or at least a reduction in HCV RNA to the level of vague before TP (Recommendation C2)
· In patients with the stage of cirrhosis in Child-Pugh, the PVT can be considered individually in highly specialized centers, preferably in patients with favorable response predictors (Recommendation C2)
· Patients with the stage of cirrhosis with Child-Pew conducting PVT is not recommended, since it is associated with a high risk of life-degrading complications (Recommendation A1)
· Treatment can be started with low doses of the Ognifun and RBV, followed by an increase in dose or with a complete dose. In the latter case, a dose reduction and treatment breaks will be required in more than 50% of cases (Recommendation A2)
Patients after liver transplantation
The progression of the liver disease in patients after TP and repeated infection occurs faster, and one third of the recipients for 5 years after TP develops the CPU. Successfully spent PVT has a positive effect on the preservation of the grafta and the patient survival.
· Patients after liver transplantation, in the case of histological confirmation of HSS, it is necessary to consider the possibility of appointing PVT (Recommendation B2) The presence of pronounced fibrosis or portal hypertension after 1 year after TP are predictors of the rapid progression of the disease and loss of the graft, in which case the PVT must be carried out as Previously (recommendation B2)
· Patients infected with a virus 1 of the genotype can be appointed without interferon therapy with direct antiviral agents. The recommended duration of treatment of patients with normal liver function and fibrosis stage 2 and below the Metavir scale after liver transplantation using D + ODA in combination with ribavirin is 24 weeks, regardless of the subtype 1 of the GSU genotype. When applying D + OPR with calcineurine inhibitors, a dose correction of calcineurine inhibitors is necessary. In clinical studies in patients after the liver transplantation, the dose of RBV was individually selected, which ranged from 600 mg to 800 mg per day.
· The liver biopsy should be carried out every time with a worsening of the FPP during PVT (C2 Recommendation)
Patients with co-infection HIV
The progression of the liver disease occurs faster under HCV / HIV co-infection, especially at a low level of CD4 cells and a weakened immune system. For this reason, in patients with KGB / HIV infection, it is necessary to consider the possibility of earlier ARVT.
· Indications for PVT assignment to patients with HCV / HIV infection are similar to testimony for patients with monoinfection of HCV (Recommendation B2)
· For patients with KGS / HIV infection, the same PVT schemes based on PVGIFN-α can be used as patients with monoinfection of HCV (Recommendation B2). It should be borne in mind that the reduction in therapy time in patients with HGS caused by a virus 1 of the genotype, up to 24 weeks is not allowed
· Patients infected with HIV and HCV 1 genotype can be considered as candidates for destination of triple therapy, but special attention should be paid to preventing unwanted drug interactions (recommendation B1)
· Patients with CD4 lymphocytes\u003e 500 cells / μl is prescribed only by PVT HGS
· With a decrease in the number of CD4 lymphocytes<350 клеток/мкл возможно одновременное назначение АРВТ и ПВТ, но необходимо учитывать возможное лекарственное взаимодействие и усугубление нежелательных побочных явлений
· In the case of pronounced immunodeficiency (CD4 lymphocytes<200 клеток/мкл), следует начать с АРВТ и после повышения иммунитета (CD4 лимфоциты >350 cells / μl) can be connected to PVT
· During the treatment of HSS, PEGIFN and RBV cannot be used in ARVT Zidovudine (AZT), staudine (D4T) and Danosin (DDI) schemes.
· Triple therapy with SMV can be used with the following ARV drugs without a dose correction: Railprivirin, ReltEgravir, Maravirock, Tenofovir, Abacavir, Zidovudine, Emitcytabine, Studyne, Didanosin and Lamivudine
· With the simultaneous use of a combination of D + ODA and ARW, it is necessary to be guided by the instructions for use on the subject of drug interactions and dosing regimen
· Perhaps earlier (CD4 lymphocytes\u003e 350 and<500 клеток/мкл) назначение АРВТ пациентам с ко-инфекцией ВИЧ/ВГС, учитывая взаимоотягощающее действие вирусов на течение обоих заболеваний (в случае принятия соответствующих рекомендаций в Национальном протоколе по АРВТ при ВИЧ-инфекции)
Patients with co-infection HBV
More often in patients with HCV / HPV infection, HBV DNA is low or indefinable. Despite the fact that this indicator may vary widely, HCV is usually the main activity factor in Hg
· Patients should be treated by Peregifn-α, RBV and PI on the same rules as patients with monoinfection of HCV (recommendation B2)
· If the VGV replication is at a considerable level before, during or after Eradication of HCV, nucleoside / nucleotide analogues can be assigned (Recommendation C2)
· The duration of the therapy of the PAGIFN-α in this category of patients should be consistent with the relevant standards for the treatment of CGV
Patients with chronic kidney disease / hemodialysis
HCV Infection is the most common in patients on hemodialysis, and is associated with an increased risk of overall death and mortality associated with liver disease. Modification of doses of drugs, depending on the renal function, is shown in Table 13.
· Patients on hemodialysis, especially those who plan to transplanted kidney, should be considered as candidates for PVT (Recommendation A2)
· PVT should include runifun-α in a reduced dosage (recommendation A1)
· RBV can be used in reduced doses with caution (recommendation B2)
· Correction of the dose of SimePrevir in patients with impaired kidney function of mild and moderate severity is not required. The safety and efficacy of the drug in patients with a violation of the function of the kidney of a severe (creatinine clearance is less than 30 ml / min) or the terminal stage of chronic kidney disease, including patients on hemodialysis, has not been studied.
Table 13. Modification of the dose of drugs depending on the renal function
Patients with transplantation of other organs
· Before the transplantation of PVT kidney can prevent the mortality in patients associated with the damage to the liver in patients after transplantation and specific causes of the renal graft dysfunction. If the possibility of PVT should be carried out in potential recipients before kidney transplantation (recommendation B1)
· After the PVT transplantation based on the runifun-α is associated with a significant risk of rejection of the graft and can be assigned only if there are strict (vital) indications, for example, aggressive cholestatite vents (Recommendation A1)
Patients actively consumed by drugs or constant replacement therapy
· PIN must be regularly and voluntarily test for the presence of Anti-HCV and, in the event of a negative result, at least every 6-12 months (recommendation B1)
· PIN should be consulted in relation to the abstinence from drug use (recommendation B1)
· IDUs must be consulted in relation to abstinence from alcohol use (Recommendation A1)
· IDUs can be included in the integrated harm reduction programs implemented on the territory of the Republic of Kazakhstan, including in places of imprisonment (recommendation B1)
· The use of injecting drugs in the past or at the time of the start of treatment is not associated with a decrease in WEVV, and the decision to treatment should be made individually (recommendation B1)
· In addition to medical reasons, before deciding on the implementation of PVT, it is necessary to assess the social factors and the predicted patient commitment to therapy (Recommendation A1)
· Training before treatment should include a discussion of methods of transmission of HCV, risk factors for the progression of fibrosis, methods of treatment, risk of re-infection and harm reduction measures (recommendation B1)
· PVT in this category of patients should be conducted by a multidisciplinary team with the participation of psychiatrist / narcologist (Recommendation A1)
· Individually, direct antiviral agents can be used in PINs located on OBT (recommendation B1). In this case, it is necessary to monitor the signs of opioid toxicity or abstinence (recommendation B1)
· OST is not a contraindication to liver transplantation (Recommendation A1)
Patients with hemoglobinopathy
The most common hemoglobinopathy associated with HSS is thalassemia at which frequent blood transfusion is required. In several published reports on clinical research, such patients traced a higher frequency of anemia during the treatment of PERSIFN and RBV. Therefore, they can be treated with standard combination therapy, but such complications as anemia should be under strict control using growth factors and blood transfusions if necessary.
HSS is also often observed in persons having a sulfur-cell anemia. With regard to this population, no results of clinical studies were published using PVT. Individual cases were successfully treated with the help of the Sagin and RBV.
Observation of patients who have not yet received treatment or in which previous therapy was unsuccessful
Patients who have not yet received treatment or in which previous therapy was unsuccessful, should be under constant supervision. The reasons for which the patient did not receive treatment, as well as the reasons for the ineffectiveness of treatment should be documented. In the event of non-efficiency of double or triple therapy, it is necessary to clearly document the version of the virological response to therapy.
· Patients with HSS, who have not passed the course of treatment, and those who have no response to previous therapy must be under constant medical supervision (Recommendation C2)
· Non-invasive methods for diagnosing the stage of fibrosis are best suited for dynamic patient monitoring (Recommendation C2)
· Screening MCC should be held regularly (Recommendation A2) with an interval of 6 months at HGS without CPU and every 3 months - in cases of CPU
· In general, this category of patients it is advisable to conduct a dynamic examination, including a platelet count, FPP, AFP, Ultrasound of the ORP, indirect elastography of the liver (with the exception of patients with verified CPU), EGDS (with CPU)
Pregnant women with hss.
· Anti-HCV carrier frequency in pregnant women in the population of Kazakhstan does not exceed 2%
· The presence of a chronic HCV infection with compensated liver disease is not a contraindication for having pregnancy, natural delivery and breastfeeding
· The risk of infection of children born from mothers infected with HCV is 1-5%
· PVT during pregnancy is absolutely contraindicated
Medical treatment rendered on an outpatient level.
Table 14. List of basic medicines required on an outpatient level
| MNN |
Pharmacotherapeutic Group |
| Pegylated alpha-2a interferon |
Interferons. PBX code L03Av11 |
|
Pegylated Interferon alpha-2b |
Interferons. PBX code L03AB10 |
| Ribavirin |
Direct action antiviral drugs. Nucleosides. PBX code J05AB04 |
| SimePrevir |
Direct action antiviral drugs. Protease inhibitor Code ATC J05AE14. |
|
Dasabuvir, Obitasvir + Paritaprevir + Ritonavir |
Direct action antiviral drugs. Dasabuvir: Nanucleosid NS5B polymerase inhibitor Obitasvir: NS5A protein inhibitor Paritaprevir: NS3 / 4A protease inhibitor Ritonavir: Pharmacokinetic booster Code ATX J05A. |
Table 15. List of additional drugs needed on an outpatient level
| MNN |
Pharmacotherapeutic Group |
| Elrombopag |
PBX code B02BX05 |
| Ursodeoxycholic acid |
A05AA02 PBX code |
| Cetirizin |
PBX code R06AE07. |
| Tofizopam |
N05BA23 PBX code |
| Citalopram | |
| Levothyroxin sodium |
Thyroid PBX code H03AA01 |
|
Paracetamol |
Npvp |
Medical treatment provided at the stationary level
The list of basic drugs corresponds to such for an outpatient level (Table 14)
Table 16. List of additional drugs required at the stationary level
| MNN |
Pharmacotherapeutic Group |
| Filgrastim |
Hematopoiesz Stimulators (Lakeopoies) PBX code L03AA02. |
| Erythropoietin Alfa. |
Code PBX B03XA01 |
| Epoetin Beta |
Hematopoiesis Stimulants (Erythropoese) Code PBX B03XA01 |
| Elrombopag |
HEMOPOESHESE STYS, THROMBOPOELES PBX code B02BX05 |
| Ursodeoxycholic acid |
The drug affecting the liver functions A05AA02 PBX code |
| Cetirizin |
Antiallergic means - H1- Blocker histamine receptors PBX code R06AE07. |
| Tofizopam |
Anxolytic remedy (tranquilizer) N05BA23 PBX code |
| Citalopram | Selective inhibitor of serotonin reverse capture code N06AB04 |
| Levothyroxin sodium |
Thyroid PBX code H03AA01 |
| Ciprofloxacin |
PBX code S01AE03. |
| Ciprofloxacin |
Antibacterial drug, fluoroquinolone PBX code S01AE03. |
| Levofloxacin |
Antibacterial drug, fluoroquinolone PBX code J01ma12 |
| Levofloxacin |
Antibacterial drug, fluoroquinolone PBX code J01ma12 |
| Ceftriaxon |
Antibacterial drug cephalosporin row J01DD04 PBX code |
| Meropem |
Antibacterial drug Carbapenes PBX code J01DH02. |
|
Paracetamol |
Npvp |
Other types of treatment
Adewant therapy
During antiviral therapy in some cases, the prescription of drugs is required to correct its side effects (for example, paracetamol, L-thyroxine, antihistamine, antibacterial agents, antidepressants, as well as growth factors, especially in patients with liver cirrhosis).
In patients with phenomena of intrahepatic cholestasis, the use of ursodeoxycholic acid (500 mg- 1000mg per day) is substantiated. · Penal liver biopsy;
· The initial period of double antiviral therapy, especially in patients with predicted by-phenomena;
· The initial period of triple antiviral therapy;
· Side effects as a result of antiviral therapy (cytopenia, infection, psycho-neurological disorders and other side effects of medium and severe).
Prevention
Preventive actions
Primary prophylaxis
Vaccine against HCV at the moment is not developed. The risk of infection can be reduced by avoiding the impact of such factors as:
· Drug consumption
· Conducting non-medical invasive manipulations (tattoo, piercing, manicure, pedicure, etc.)
· Joint use (including family members) personal hygiene and care objects that can be contaminated with infected blood (scissors, razors, toothbrushes, etc.)
· Disorder sex with unprotected sex with hepatitis with persons infected with hepatitis
· Blood donation and organs infected with HCV
· Conduct medical invasive manipulations in improper processing of equipment and materials (acupuncture, dental and cosmetology manipulations, hirudotherapy, etc.)
· Excessive use of invasive medical manipulations (injections, infusion, plasmapheresis, endoscopic and surgical interventions)
· Transfusion of unsafe blood products
· Safety non-compliance with medical workers
Secondary and tertiary prevention
For people infected with the hepatitis C virus, the following measures are recommended:
· Obtaining information and consulting with regard to transmission of infection, methods of prevention, medical care and treatment
· Immunization of hepatitis A vaccines and in
· Regular control (accounting at the place of residence) and obtaining timely and appropriate medical care, including, if necessary, antiviral therapy
· Exception / correction of factors for the progression of chronic liver disease (drug consumption, alcohol, tobacco, overweight, IR, SD, co-infection HIV)
Further maintenance
Further maintenance of patients who reached WEV
· Patients who have achieved WEVO should define HCV RNA and the ALC activity in 48 weeks after the end of treatment. In the event of a negative result of PCR and normal transaminase indicators, monitoring patients who do not have CPU may be discontinued (C2 recommendation)
· Patients with the CPU, which reached WEVO, it is necessary to continue screening for the presence of the ICC at least than every 6 months (recommendation B1)
· The frequency of re-infection after the successful treatment of HCV among high-risk groups, such as PIN, is 1-5% per year. PINs who have reached WEV, and continuing surfactant consumption, need an annual screening for HCV RNA (recommendation B2)
· Since hypothyroidism may arise after the end of treatment, it is necessary to check the level of TSH after 1 and 2 years.
Information
Sources and literature
- Protocols of the meetings of the Expert Council RCRs MZSR RK, 2015
- List of references: 1) WHO GUIDELINES FOR THE SCREENING, CARE AND TREATMENT OF PERSONS WITH HEPATITIS C INFECTION 2014. WHO PUBLICATION. http://apps.who.int/iris/bitstream/10665/111747/1/9789241548755_eng.pdf?ua\u003d1&ua\u003d1 2) Easl Clinical Practice Guidelines. Management of Hepatitis C Virus Infection. Journal of Hepatology 2011; 55: 245-264 3) Easl Clinical Practice Guidelines: Management of Hepatitis C Virus Infection. Journal of Hepatology 2014; 60J: 392-420 4) Easl Recommendations on Treatment of Hepatitis C 2015. Journal of Hepatology 2015; http://www.easl.eu/medias/cpg/hepc-2015/full-report.pdf 5) AASLD Diagnosis, Management and Treatment of Hepatitis C: An Update. Hepatology 2009; 49 (4): 1335-1374 6) Treatment of Genotype 1 Chronic Hepatitis C Virus Infection: 2011 Practice Guideline by The American Association For the Study of Liver Diseases, Hepatology 2011; 54 (4): 1433-1444 7) AASLD-IDSA Recommendations for Testing, Managing, And Treating Hepatitis C 2014. http://www.hcvguidelines.org/fullReport 8) AASLD-IDSA AN UPDATE TO THE RECOMMENDATIONS FOR TESTING, MANAGING, AND TREATING HEPATITIS C 2014 http: // www.hcvguidelines.org/full-Report-View 9) An Update On The Management of Chronic Hepatitis C: Consensus Guidelines from The Study of the Liver. CAN J Gastroenterol 2012; 26 (6): 359-375 10) Protese Inhibitor-based Triple Therapy In Chronic Hepatitis C: Guidelines by The Studch Association For the Study of the Liver. Liver International 2012; 32 (10); 1477-1492 11) UK CONSENSUS GUIDELINES FOR THE USE OF THE PROTEASUS INHIBITORS BOCEPREVIR AND TELAPREVIR IN GENOTYPE 1 CHRONIC HEPATITIS C INFECTED PATIENTS. Alimentary Pharmacology and therapeutics 2012; 35 (6): 647-62 12) Treatment of Chronic Hepatitis C GENOTYPE 1 With Triple Therapy Comprising Telaprevir or BocePrevir. Swiss Association for the Study of the Liver. Swiss Medical Weekly 2012; 142: W13516 13) Russian recommendations for the diagnosis and treatment of adult patients with hepatitis from 14) European AIDS Clinical Society (EACS) Guidelines for the Treatment of HIV, HIV and HEPATITIS C CO-INFECTION, AND HIV WITH OTHER CO- Morbidities 2013; Version 7 15) Instructions for medical use of drugs: Ribavirin, Ognifn-α 2A, PEREGIFN-α 2B, SimePrevir, Dasabuvir combination with ombitasvir, parityrevir, ritonavir.
Information
List of protocol developers:
1) Nersesov Aleksandr Vitalyevich - Doctor of Medical Sciences, Professor, RGP on the PCB "Research Institute of Internal Diseases and Cardiology" MZSR RK, Head of the Department of Gastroenterology and Hepatology with Endoscopy Course, Chairman of the Kazakh Liver Study Association.
2) Kaliaskarov Kulpash Sagyindikovna - Doctor of Medical Sciences, Professor JSC "National Scientific Center of Oncology and Transplantology", Chief Freelance Hepatologist / Gastroenterologist MZSR RK.
3) Jumabaeva Algall Yerkenovna - Master of Public Health of the RGP on the PCB "Research Institute of Internal Diseases and Cardiology" MZSR RK, Assistant Department of Gastroenterology and Hepatology with Endoscopy Course, Secretary of the Kazakh Association for Liver Study.
4) Tabarov Adlet Berikbolovich - RSP on the PVV "Hospital of the Medical Center Management of the Office of the Republic of Kazakhstan" Head of Innovation Management, Clinical Pharmacologist.
Conflict of interest:absent.
Reviewers:
1) Bakulin I.G., D.M., Professor, Head of the Research and Research Department of the Hepatology of the Moscow Clinical Scientific and Practical Center, Chief Gastroenterologist of the Health Department of the Moscow.
2) Doskeepeva S.T., D.M., Professor, Vice-Rector, Head of the Department of Infectious Diseases of the Kazakh Medical University of Continuing Education MZSR RK.
Protocol revision conditions: The revision of the Protocol 3 years after its publication and from the date of its entry into force or in the presence of new methods with the level of evidence.
________________________________________________________________________________________
Attachment 1
Rules for conducting a base biopsy liver
Conducting PBP requires compliance with the following rules:
1. Before conducting a biopsy, it is necessary to clearly formulate the indications for its implementation.
2. To all patients before performing the liver biopsy should be the ultrasound of the OBR. This study allows you to identify an anatomical version of the structure of the liver and the presence of focal formations in its parenchyma, which may require a visual biopsy under visual control.
3. During the week, before conducting puncture, it is necessary to determine the amount of platelets and prothrombin time (PV) or prothrombin index (PI).
· If the number of platelets is ≥90,000 / mm3, then manipulation can be performed by a routine method (percutaneous liver biopsy)
· If PV is lengthened in less than 3 seconds. in comparison with the control value (provided by the laboratory in which the blood sample study is carried out), pi at least 70%, thrombin time (TV) and activated partial thromboplastin time (AFTT) do not exceed 1,5 norms, the biopsy can be carried out percutaneous access
· In all other cases, the decision on the implementation of the liver biopsy is made on an individual basis by estimating benefits and risk from the planned manipulation. In the event of a strict need to carry out a liver biopsy in patients with hypocoagulation or low platelets in some cases, replacement therapy can be justified.
4. Before the biopsy it is necessary to sign an informed consent in a patient in which the manipulation technique and possible complications are available.
5. During the execution of the biopsy, the doctor and patient must be in constant contact. The patient is clearly and in a timely manner must execute the commands of the doctor. With elevated patient's excitability and the absence of signs of hepatic insufficiency, sedatives are possible.
6. The choice of needle for biopsy is advisable to carry out the personal experience of the operator. In everyday practice, the needles of Mengini and Tru-Cut needles are convenient.
7. Doctors whose personal experience does not exceed 20 manipulations, perform biopsy in the presence and under the control of a more experienced doctor in a specialized hepatological center.
8. Biopsy is performed under the control of ultrasound, which minimizes the number of complications
9. In the case of an "empty" biopsy (failed to obtain a fabric or its amount is not enough for a morphological study), especially in patients with severe fibrosis tissue or cirrhosis, it is possible to simultaneously carry out a re-fence that is not accompanied by an increase in the risk of complications.
10. The active observation of patients for 8 hours and first night after manipulation (with the implementation of ultrasound, general blood test) should be carried out in a medical organization. Assessment of the results of the PBP is carried out using semi-quantitative scales for describing the degree of non-pollial changes and the liver tissue fibrosis stages (see tables 4 and 5).
11. The correct results of the morphological research should be considered when receiving a batch of hepatic tissue at least 15 mm and the number of portal paths at least 10.
_____________________________________________________________________________
Appendix 2.
Scheme 1.

Scheme 2.

* Patients with 1A HCV genotype must be examined for the presence of NS3 Q80K polymorphism of the virus before starting therapy
** HIV / HCV-coinfected patients with liver cirrhosis previously not received treatment, and patients with preceding relapse should receive a 48-week course of therapy (12 weeks of triple therapy of Simeperevir and the next 36-weeks of dual therapy)
Scheme 3.

* Used highly sensitive method with lower limit definition<15 МЕ/мл
** Adverse factors include CMT\u003e 25, insulin resistance, metabolic syndrome, severe fibrosis or CPU
*** Patients with genotypes 2 and 3 HCV who have achieved full PPC (without BVA) and not having adverse factors can also receive therapy within 48 weeks
Scheme 4. Algorithm for the treatment of HSS caused by a virus 1 of the genotype, in non-interferonic therapy mode D + ORD

Attached files
Attention!
- By self-medication, you can apply irreparable harm to your health.
- The information posted on the MedElement website and in MEDElement mobile applications, "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Directory", cannot and should not replace a full-time doctor consultation. Be sure to contact medical facilities in the presence of any diseases or disturbing symptoms.
- The choice of medicines and their dosages should be stated with a specialist. Only a doctor can prescribe the necessary medicine and its dosage, taking into account the disease and the state of the patient's body.
- Website MedElement and Mobile Applications "MedElement (Medleylement)", "Lekar Pro", "Dariger Pro", "Diseases: Directory of Therapist" are exclusively information and reference resources. The information posted on this site should not be used for unauthorized changes to the doctor's prescriptions.
- The editorial office of MedElement is not responsible for any damage to health or material damage resulting from the use of this site.
Optimal combinations of oral instruments for the eradication of hepatitis C virus: Ribavirin's role
Christophe HEZODE 1, *, Jean-Pierre Bronowicki 2
1 Department of Hepatology and GastroNerology, Hopital Henri Mondor, AP-HP, Universite Paris-Est, Inserm U955, Creteil, France; 2 Department of Hepatology and Gastroenterology, Centre Hospitalier Universitaire de Nancy, Universite de Lorraine, Inserm U954, Vandoeuvre-Les-Nancy, France
abstract
Modern completely oral circuits without interferon provide a sustainable virological response (WSV) in 90% of cases and reduce the duration of treatment to 12 weeks. In most patients with chronic hepatitis C, including patients with cirrhosis of the liver and without it, who have not been treated earlier and have already received therapy. There are many combinations of direct-action antiviral drugs (PPPD), with which it is possible to achieve an optimal ratio of efficiency and security of therapy. Each of these these schemes can be modified according to various parameters, including the use of ribavirin (RBV). When using combinations based on SofosBuvir (SOF), the use of RBV is advisable in the following situations: in patients infected with the hepatitis C virus (HCV) of genotype 1, which have previously obtained treatment and having cirrhosis or decompensated liver cirrhosis, and in patients infected with HCV genotype 3, With cirrhosis of the liver. In these situations, adding RBV reduces the duration of treatment to 12 weeks. In most cases, leading to a decrease in its value. It is necessary to find out the need to use RBV in patients with cirrhosis of the liver, receiving the treatment of SOF and SimePrevir. RBV is recommended in the treatment of all patients infected with HCV genotype 1A receiving a combination of three PPPDs: parityrevir / ritonavir, ombitasvir, dasabuvir. In general, the addition of RBV to various PPP combinations slightly increases the risk of anemia. Nevertheless, severe anemia is rarely observed and amenable to correction by reducing the RBV dose without affecting the achievement of uvo.
Practically due to the fact that RBV is an inexpensive drug that is well tolerated when combining with interferon schemes, it remains an effective means for improving the hepatitis C and optimization of the results of their use.
© 2015 European Association for the Study of the Liver.
Keywords: ribavirin, antiviral drugs of direct action, without interferon, SofosBuvir.
Reduction: ASV - ASUNAPREVIR; APRI is the AspartataminTransferase Index / platelets; DCV - Daclatasvir; HCV - Hepatitis C virus; IFN - Interferon; LDV - Ladipasvir; Pegifn - peginterferon; RBV - Ribavirin; SMV - SimePrevir; SOF - SofosBuvir; GTF - Guanozintrifhosphate; IMFDG - inosine monophosphate dehydrogenase; PPPD - antiviral drugs direct action; UVO is a steady virological response; HGS - Chronic Hepatitis C.
Introduction
Chronic hepatitis C (HSS) flows with the progressive lesion of the liver, which can lead to the development of cirrhosis and hepatocellular cancer. According to modern estimates, the HSS suffers about 130-150 million people, mortality from it is 350,000 cases per year. Today 7 genotypes of hepatitis C virus (HCV) are allocated, of which the most common worldwide is genotype 1.
For the treatment of HSS, the SOPOSBUVIR (SOF) is currently applied, an analogue of urididium nucleotide, which suppresses the non-structural protein of polymerase 5B (NS5B) and is used in combination with other drugs, including pegylated nonerferon (Pegifn), Ribavirin (RBV) and antiviral direct operations (RBV PPPD). The use of non-interferon schemes based on SOF leads to an increase in the frequency of a sustainable virological response (WSV) more than 90% against the background of reducing the duration of treatment (? 12 weeks). Approval and other non-interferon schemes are expected based on the results of studies of the III phase, in which the same effectiveness was detected as non-interferon schemes containing SOF.
Combined therapy with the use of RBV made it possible to significantly increase the frequency of response to Pegifn due to the prevention of relapses. RBV was an important component of PEGIFN-based schemes, which included inhibitors of the first generation protease, used to prevent the virological breakthrough or relapse, but the results of studies of the phase II devoted to the study of schemes without interferon based on PPTs indicate that the inclusion of RBV is required always . Despite the fact that RBV is characterized by less pronounced toxicity in the absence of pegifn, it is teratogenic and causes the development of hemolytic anemia. Thus, the purpose of this review was to identify groups of patients for whom recommendations on the use of RBV are preserved as part of various PPP schemes already approved today or the approval of which is expected in the near future.
Ribavirin action mechanism
The disappearance (cure) of infected cells (the second phase of the curve) against the background of antiviral therapy occurs under the influence of a plurality of parameters, some of which can be modified to optimize the response to treatment. These include antiviral efficacy of the combination of drugs, the duration of treatment and the use of RBV. Thus, patients with a slow decrease in curve in the second phase (such as patients with adverse genotype IL28B, liver cirrhosis, HCV genotype 3 or 1a, etc.) requires the use of a scheme with a more pronounced antiviral efficiency during the corresponding period of time. In addition, the use of RBV can be effective both to reduce the duration of treatment and to increase the frequency of WSV as a given duration of therapy. This is due to the acceleration of the second phase of reducing the viral load against the background of RBV by means of still not installed mechanisms in patients who have achieved efficient suppression of the virus products using non-interferon schemes.
It was found that RBV may cause a pronounced, moderate or transient antiviral effect in a significant share of patients receiving it as a monotherapy. Moreover, against the background of the RBV monotherapy, a decrease in the level of the alanine substransferase in serum was observed, which did not depend on the antiviral activity of the drug. A number of possible mechanisms for direct suppression by the drug of viral RNA polymerase are assumed. However, the moderate antiviral effect of the RBV in vivo monotherapy makes this hypothesis (direct suppression of polymerase RNA) is unlikely. It was suggested that the RBV antiviral activity is due to the depletion of the intracellular reserve of guanosynthosphate caused by the suppression of inosine monophosphate dehydrogenase (IMFDG) under the influence of the drug. However, other powerful specific inhibitors of the EMFDG used separately or in combination with RBV or IFN do not have a significant effect on HCV replication in patients with HSS. This suggests that the suppression of the IMFDG is not related to RBV antiviral activity. The HCV-infected patients receiving RBV also studied the concept of mutagenic properties of RBV, leading to the development of "error disasters", i.e., violation of the distribution of mutant options in quasivides and the emergence of generation of non-visual viral populations. In this case, conflicting results were obtained. Nevertheless, a study was recently carried out in which the analysis of RBV-induced mutations was carried out using a highly sensitive deep sequencing method. In this study, it was found that RBV has a mutagenic effect on HCV by induction of the replacement of nucleotides, due to which the RBV antiviral activity can be explained. But RBV-induced mutagenesis does not explain the development of a biochemical response. Finally, the hypothesis that RBV can act as a factor that stimulates the IFN signal path by increasing the induction of IFN-stimulated genes was not confirmed in vivo. Thus, the discrepancy between antiviral and biochemical response to RBV suggests that RBV can act through various mechanisms. At the same time, the direct antiviral effect of the drug is partly due to its mutagenic properties, and the indirect biochemical effect is implemented through an unknown mechanism.
Effect of RBV on the effectiveness of treatment in patients without liver cirrhosis infected with HCV genotype 1
SophosBuvir-based schemes
In vitro was demonstrated expressed paraenotypic activity of SOF against HCV (genotypes 1a, 1B, 2a, 2b, 3a, 4a, 5a, and 6a) in concentrations that suppress the replication of the virus by 50% equal to 0.014-0.11 μmol. In vitro studies with the use of combinations of drugs, the additive interaction of SOF and IFN was demonstrated. For a combination of SOF and RBV, only insignificant synergism was discovered. However, in the study of ELECTRON phase II, all 10 not treated earlier patients infected with HCV genotypes 2 and 3, which received the therapy of Sof + RBV for 12 weeks, reached WEV to the 24th week (UVO24). The other 10 not treated patients infected with HCV genotypes 2 and 3 were obtained by the SOF monotherapy for 12 weeks, and only 6 of them reached UVV24. In this group, all 10 patients were obtained a quick response and an undefined HCV RNA level was noted by the 4th week of treatment, which remained throughout the remaining period of treatment. In 4 patients developed recurrence after the completion of treatment. Despite the limited statistical significance of the study due to a small sample size, the results obtained emphasize the important role of RBV in the prevention of relapses and conservation of an antiviral response.
Sofosbuvir and Ribavirin
In an independent study, the effectiveness of SOF was estimated in combination with RBV within 24 weeks. In not previously treated patients infected with HCV genotype 1. In the second part of the study, 50 patients were divided into groups obtained by SOF in combination with RBV, which was appointed either depending on body weight, or in a low dose of 600 mg / day . The frequency of UVA24 was 68% in patients with which RBV was appointed depending on body weight, and only 48% in patients who received a low dose of RBV. However, given the low indicator of the ratio of efficiency / cost, the use of this strategy in patients infected with HCV genotype 1 is not recommended.
Sofosbuvir and Ladipasvir
In 3 phase III studies, the effectiveness of the SOF combination with Ladipasvir (LDV) was estimated (LDV inhibitor) with RBV and without it (1000 mg / day in patients with a body weight of less than 75 kg and 1200 mg / day in patients with a body weight of 75 kg and more ) In different groups of patients infected with HCV genotype 1 (Table 1). It is important to note that these studies did not have sufficient power to compare the responses to the application of schemes with RBV and without it or the effectiveness of therapy for 12 and 24 weeks. We have not previously obtained treatment of patients without cirrhosis infected with HCV genotype 1, SOF + LDV circuit for 8 weeks. It was also effective as the SOF + LDV scheme with RBV for 8 weeks. and SOF + LDV scheme for 12 weeks. The frequency of uvo was 94 VS 93 VS 95%, respectively. In not previously treated patients with cirrhosis of or without it, infected with HCV genotype 1, SOF + LDV circuit for 12 weeks. It was also effective as the SOF + LDV scheme with RBV for 12 weeks. and SOF + LDV or SOF + LDV + RBV circuit for 24 weeks. (99 VS 97 VS 98 VS 99%, respectively). In patients without liver cirrhosis, adding RBV did not affect IVV. The third study was estimated the effectiveness of the same schemes as in the first 2 studies, but in patients with cirrhosis or without it, which had previously received treatment. The frequency of WSVO was similar to the background of circuits with RBV (96 and 99% when used within 12 and 24 weeks. Respectively) and without it (94 and 99% when applied for 12 and 24 weeks. Respectively). In patients without liver cirrhosis, the use of RBV did not affect IVV. Based on the foregoing, in patients without a liver cirrhosis infected with HCV genotype 1, SOF and LDV can be used without RBV.
Sofosbuvir and Daktosasvir
Daclatasvir (DCV) is a powerful Pangeneotypic NS5A inhibitor with antiviral activity with respect to HCV genotypes 1-6, which is used for the treatment of XGC in combination with SOF. The effectiveness of this combination (Sof + DCV) with RBV and without it (1000 mg / day in patients with a body weight of less than 75 kg and 1200 mg / day in patients with a mass of body 75 kg or more) was studied mainly in patients without liver cirrhosis infected The genotype virus 1. Patients in randomized manner were distributed to groups received by Sof + DCV with RBV and without it within 12 weeks. (82 previously not treated patient) or 24 weeks. (41 patient who had previously registered therapeutic failure against the background of teleprierevir therapy or boraprevir in combination with IFN and RBV). In patients who did not receive previously treated, the frequency of UVO12 amounted to 100 and 95% in the SOF + DCV and SOF + DCV + RBV groups, respectively. In a group of patients who had previously registered virological failure against the background of therapy inhibitors of protease, the frequency of UVO12 was equal to 100 and 95% in SOF + DCV and SOF + DCV + RBV groups, respectively. In an uncontrolled cohort of patients in real clinical practice, the frequency of UVO4 was 100% in 20 patients with severe fibrosis (but without cirrhosis, the fibrosis stage was exhibited on the basis of non-invasive markers) infected with HCV genotype 1 receiving Sof + DCV without RBV for 12 weeks. . Due to the small number of patients who received this therapy scheme, defined conclusions regarding the efficiency of adding RBV cannot be made. Nevertheless, these preliminary results indicate the absence of the need to add RBV to this combination.
Sofosbuvir and Simeperevir
In the COSMOS study, the effectiveness of the combination of SOF and SimePrevir (SMV), protease inhibitor, with RBV or without it for 12 or 24 weeks. It was estimated in patients without severe fibrosis infected with HCV genotype 1 that had not previously received treatment or not responding to previous therapy. UVO12 was achieved in 98 (91%) of 108 patients receiving RBV, and in 56 (95%) of 59 patients who did not receive RBV. The frequency of UVO12 was similar regardless of the status of preceding therapy (38 of 40 patients who did not receive previously treated VS 116 of 127 patients who were not previously responding) and the duration of treatment (77 of 82 patients after 12 weeks. Therapy VS 77 of 85 patients after 24 Ned. Therapy). Nor RBV nor the duration of therapy did not have a clear effect on the frequency of WEV in patients infected with HCV with GLN80LYS polymorphism at the beginning of the study. The high frequency of WEVS in patients infected with HCV genotype 1A, regardless of the presence of GLN80LYS polymorphism at the beginning of the study, and in patients infected with HCV genotype 1b. These results were confirmed in a clinical study of the III phase, which was attended by patients without a liver cirrhosis. Thus, the addition of RBV apparently does not increase the effectiveness of therapy in patients without severe fibrosis, regardless of the status of previous therapy or subtype HCV. This combination can be recommended as a scheme without RBV for all patients infected with HCV genotype 1, especially for patients without a liver cirrhosis.
Paritaprevir-based schemes
The ABBVIE scheme includes a combination of parityrevir (previously ABT-450) / Ritonavir with Obitasvir (previously ABT-267) in fixed doses as part of one dosage form and dasabuvir (previously ABT-333) (3-PPT) with RBV, assigned depending on the mass Body (1000 mg / day in patients with body weight less than 75 kg and 1200 mg / day in patients with a mass of body 75 kg or more), or without it. Paritaprevir, NS3 / 4A HCV protease inhibitor with power in nanomolar in vitro concentrations, is assigned simultaneously with low doses of ritonavir (parityrevir / ritonavir), the CYP3A4 inhibitor, which in itself does not have antiviral activity. The ombitasvir is an NS5A HCV inhibitor with a power in piquetural concentrations in vitro, and dasabuvir is an NS5B HCV polymerase RNA inhibitor with a power in nanomolar in vitro concentrations. In 4 phase III studies, the effectiveness of the 3-PDAP scheme was studied in different groups of patients infected with HCV genotype 1, including patients without liver cirrhosis that did not earlier treatment, and patients without a liver cirrhosis previously obtained by therapy Pegifn and RBV (Table 2). It is important to note that these studies did not have sufficient power to compare the responses to therapy with the use of RBV and without it.
The placebo-controlled study was attended by 631 patients without a liver cirrhosis infected with HCV genotype 1 and not previously obtained treatment. In this study, on the background of therapy according to the 3-PPT + RBV scheme for 12 weeks. There was a high frequency of UVV12, equal to 96.2% (455 of 473). This indicator was almost the same in patients infected with HCV genotypes 1A (95.3%; 307 of 322) and 1b (98%; 148 out of 151). On the basis of these data, 2 major phase III studies were developed to assess the effect of RBV in combination with 3-PDAPs when applied for 12 weeks. The effectiveness and safety of therapy in patients without a liver cirrhosis infected with HCV genotype 1a or 1b that have not received previously treated treatment. In these studies, high VSV12 indicators were obtained, equal to 99.5 (209 of 210) and 99.0% (207 of 209) in patients infected with HCV genotype 1b, against the background of adding RBV and without it, respectively. This suggests that RBV does not increase the response rate in patients with HCV infection of genotype 1b, which allows them to apply the scheme without RBV. In patients infected with HCV genotype 1a, the high frequency of WEVS was observed as against the background of the use of RBV (97%; 97 out of 100) and without it (90.2%; 185 of 205). In a group without RBV, a higher frequency of virological failures was observed (7.8 Vs 2.0%). The difference between groups suggests that RBV helps to increase the effectiveness of treatment in patients infected with HCV genotype 1A, which allows us to recommend a 3-PPP + RBV scheme as an optimal treatment method for these patients.
In a placebo-controlled study, which was attended by patients who have previously received treatment, which was assigned therapy under the 3-PPT + RBV scheme for 12 weeks, the frequency of UVO12 was 96.3% (286 of 297). The frequency of virological failures was almost the same among patients infected with HCV genotypes 1A and 1B: 2.9 (5 of 173) and 1.6% (2 of 123), respectively. The frequency of UVO12 was similar regardless of the status of preceding therapy: 95.3 (82 of 86), 100 (65 of 65) and 95.2% (139 out of 146) in patients who have developed a relapse, patients who have achieved a partial response and not Answered response, respectively. Based on these data, the advantage of the RBV inclusion in the 3-PPP scheme was estimated solely in the HCV-infected HCV genotype 1b of patients without cirrhosis previously received by pegifn and RBV therapy. These patients were randomized to be divided into groups that received treatment according to the 3-PDAP scheme for 12 weeks. with RBV or without it. In a group that did not receive RBV, the frequency of UVO12 was 100% (91 of 91), which was no less than in a group obtained RBV (97%; 85 of 88). Virological failures during treatment was not registered. Scheme with 3-PPT for 12 weeks. It is sufficient to achieve an optimal response to the treatment of patients without cirrosis infected with HCV, previously obtained pegifn and RBV therapy. Based on the foregoing, a 3-PPT scheme without RBV for 12 weeks. It is the optimal method of treating patients infected with HCV genotype 1b. Its use is accompanied by a high frequency of HCV eradication. The patient with the HCV infected HCV genotype 1a requires the appointment of the full dose of RBV to maximize the chances of the virus eradication.
Daclatasvir-based schemes
For the treatment of chronic hepatitis C DCV was appointed with SOF and in combination with other PPAP. In the randomized open study of the phase II, the effectiveness of 12 and 24-week schemes, which included low doses of DCV (30 mg / day) + SMV (NS3, 150 mg / day protease inhibitor) with RBV or without it (1000 mg / day in patients With a body weight of less than 75 kg and 1200 mg / day in patients with a body weight of 75 kg or more), in patients with chronic HCV infection of genotype 1, which did not basically have a liver cirrhosis. From patients with HCV genotype 1b 84.9 and 74.5% of patients who have not received previously treated, and 69.6 and 95.0% of patients who did not have the answer not previous therapy reached UVV12 on the background of DCV + SMV without RBV and with RBV, respectively. The duration of the response did not have a significant effect on its frequency. Adding RBV to the DCV + SMV scheme also practically did not affect the WSV12 indicators: in patients who did not receive previously treated, there was no increase in the frequency of UVV12 against the background of RBV, whereas in a smaller subgroup of patients who did not reach the response to previous therapy, the frequency of UVO12 RBV background was higher. Among patients with HCV genotype 1A, the application of the DCV + SMV scheme with RBV has led to a response to 66.7% of cases in patients who have not received previously treated, and was ineffective in patients who have not achieved an answer to previous therapy.
ASUNAPREVIR (ASV) is an NS3 protease inhibitor, active against genotypes 1, 4, 5 and 6 in vitro. With a preliminary clinical assessment of the DCV + ASV combination, high VSV indicators in patients infected with HCV genotype 1b were obtained. However, the effectiveness relative to the genotype 1a was limited. In this regard, in a major clinical study of the III phase, the safety and efficiency of the administration of the oral combination of DCV + ASV without RBV was studied within 24 weeks. In patients infected with HCV genotype 1b (including patients with cirrhosis of the liver) who had not previously received treatment under the response to the previous pegifn + RBV therapy, or having medical contraindications to the use of pegifn + RBV, and / or poorly tolerated This scheme is previously. The IVV frequency in this study ranged from 82% in patients who had previously had a response to therapy, up to 91% in patients who had not received treatment. One of the disadvantages of this study is the lack of a group in which RBV would be added to the treatment regimen. It is possible that the addition of RBV could increase the effectiveness of treatment in subgroups of patients with the lowest uvo frequency against the background of this two-component scheme. It is interesting to note that the purpose of DCV and ASV with Pegifn and RBV for 24 weeks. It was accompanied by a high frequency of UVV12 (98.9%) in patients infected with HCV genotype 1b, not responding to previous therapy. This indicates the advantage of additional treatment in this group of patients who are poorly treatable.
The combination of three antiviral drugs with a different mechanism of action also contributes to an increase in the barrier of resistance and can increase the effectiveness of treatment. In this regard, the fully oral combination of DCV, ASV and BECLBUBUBUP (BMS-791325), the nanucleoside polymerase inhibitor in the "thumb" was successfully tested (the frequency of UVO12 92%) in the phase II study. Based on the results obtained, a study of phase III was developed to evaluate the effectiveness of this fully oral combination without RBV in patients without a liver cirrhosis infected with HCV genotype 1 that have not received and have previously received treatment. In general, UVV12 reached 91% of patients. At the same time, a higher frequency of WEVO was observed in patients infected with HCV genotype 1A compared to 1B genotype (100 VS 85-90%), which indicates the need to study the effectiveness of RBV-containing schemes in patients infected with HCV genotype 1A. However, due to problems with the security of Bristol-Myers Squibb, it was recently decided not to register this combination in American (FDA) and European (EMEA) drugs on drugs.
Effect of RBV on the effectiveness of treatment in patients with liver cirrhosis infected with HCV genotype 1
SophosBuvir-based schemes
Sofosbuvir and Ladipasvir
The effectiveness of the SOF + LDV scheme with RBV or without it (1000 mg / day in patients with a body weight of less than 75 kg and 1200 mg / day in patients with a body weight of 75 kg or more) for 12 or 24 weeks. It was estimated from the previously obtained treatment of patients infected with HCV genotype 1, with cirrhosis of the liver or without it. In patients with cirrhosis (stage F4 on the Metavir scale or estimate 5-6 on the ISHAK scale; Evaluation of Fibroscan\u003e 12.5 kPa or Evaluation of Fibrotest\u003e 0.75 and Apri\u003e 2) The frequency of UVV12 amounted to 100% on the background of applying SOF + LDV scheme With RBV for 12 or 24 weeks. and 94% against the background of treatment according to the SOF + LDV scheme for 12 or 24 weeks. This indicates the positive effect of RBV, as well as that the SOF + LDV + RBV scheme for 12 weeks. It is optimal for patients with cirrhosis of the liver infected with HCV genotype 1, not previously obtained treatment (see Table 1). In another study, the same 4 groups were estimated with the same definition of the liver cirrhosis, as in the previous study, but in patients who have previously received treatment, with cirrhosis of the liver without it. The frequency of WSVO was almost the same in all groups. However, it was somewhat lower in patients with cirrhosis received treatment within 12 weeks. With the addition of RBV (82%) and without it (86%), compared with patients treated within 24 weeks. Using RBV and without it (100% in both groups) (see Table 1). The results of the analysis of data obtained in 513 patients with cirrhosis included in different studies of the II-III phases in which the effectiveness of the combination of SOF + LDV was evaluated, indicate that the use of SOF + LDV for 12 weeks. It may be sufficient for the treatment of patients infected with HCV genotype 1 that have not received previously treated. On the other hand, the frequency of UVO12 against the background of the use of SOF + LDV for 12 weeks. In patients with cirrhosis, which have previously received treatment, was equal to 90% compared with 96% against the background of the treatment according to the SOF + LDV + RBV scheme for 12 weeks. and 98-100% with the use of SOF + LDV within 24 weeks, with RBV or without it. Thus, the SOF + LDV + RBV scheme for 12 weeks, possibly the most efficient and cost-effective method of therapy that previously received patients with cirrhosis of the liver infected with HCV genotype 1. This assumption is also confirmed by the results of the Sirius study, which was compared The effectiveness of the application of the SOF + LDV + RBV circuit for 12 weeks. and combinations of SOF + LDV within 24 weeks. In patients with cirrhosis of the liver, infected with HCV genotype 1, not previously responding to the therapy inhibitors of the first generation protease inhibitors (in both groups, the frequency of UVO12 was 95%). Unfortunately, in this study, the effectiveness of the SOF + LDV scheme with RBV for 12 weeks was not estimated. The frequency of UVO12 in 20 patients infected with HCV genotype 1, with cirrhosis (stage B on the Child-Pugh scale) against the background of the use of SOF + LDV for 12 weeks. Almost 65% was equal. In another study, the effectiveness of the SOF + LDV scheme with RBV for 12 weeks. Compared with the effectiveness of the same scheme within 24 weeks. In patients infected with HCV genotype 1, with cirrhosis (stage B and C on the Child-Pugh scale). The data obtained recently in uncontrolled cohort in real practice indicate that the use of this scheme for 12 weeks. With RBV (164 patients) and without RBV (21 patients) in patients with decompensated cirrhosis of the liver, infected with HCV genotype 1, led to the achievement of WSV in 86 and 81% of cases, respectively. Some increase in efficiency in the RBV group may indicate in favor of its purpose to patients with HCV genotype 1. Thus, the use of RBV can reduce the duration of therapy to 12 weeks. In patients with cirrhosis of the liver, which have previously received treatment. Its use is recommended in patients with decompensated cirrhosis. Probably, the general conclusion is that adding RBV to the SOF + LDV scheme assigned to 12 weeks, allows you to increase the frequency of IVV.
Sofosbuvir and Daktosasvir
In a clinical study of the II phase, the number of patients with liver cirrhosis was extremely limited, the effectiveness of a shorter course of therapy (12 weeks) was not evaluated in patients previously failed against the background of the use of protease inhibitors. This indicates that the potential role of RBV is clearly not established and requires additional data from clinical studies or real cohort. The effectiveness of the application of the SOF + DCV circuit for 12 and 24 weeks. With RBV or without it, it was studied on the basis of data obtained in a major cohort in a real clinical practice, which included patients with cirrhosis (the diagnosis was established on the basis of non-invasive markers) infected with HCV genotype 1. This study was not controlled, and the choice of treatment regimen was carried out. At the discretion of the doctor. In this regard, it is difficult to make certain conclusions regarding the use of RBV and the optimal duration of treatment in this population. Nevertheless, the frequency of UV4 was 76.5 (26 of 34), 100 (9 of 9), 94 (203 of 216) and 98.3% (59 out of 60) in patients who received treatment for this scheme with RBV and without It for 12 weeks, and in patients who received the same therapy within 24 weeks., respectively. Based on preliminary data, it can be concluded that RBV can reduce the duration of treatment up to 12 weeks. In this population. Nevertheless, additional data are required regarding patients receiving Sof + DCV with RBV for 12 weeks. The effectiveness of this scheme was estimated in 45 patients with decompensed cirrhosis of the liver infected with HCV genotype 1 included in the uncontrolled study of the III phase. The initial dose of RBV was equal to 600 mg per day. This dose rose to 1000 mg per day, taking into account the level of hemoglobin and kidney function. The total frequency of UVO12 amounted to 82%. The treatment was not equally effective in patients with the stages of the zirrosis A and B (\u003e 90%) and with the ST stage (< 60 %) по шкале Чайлда-Пью. Это позволяет предположить, что применение схемы SOF + DCV с RBV (с повышением дозы) в течение 12 нед. является оптимальным методом лечения больных с декомпенсированным циррозом печени в стадиях A и B по шкале Чайлда-Пью, инфицированных HCV генотипа 1 . Комбинация SOF + DCV с RBV (45 пациентов) и без него (5 пациентов) назначалась на 12 нед. больным с циррозом печени, инфицированным HCV генотипа 1, вошедших в реальную неконтролируемую когорту. Частота УВО равнялась 82 и 60 % на фоне применения RBV и без него соответственно . Небольшой выбор участников, а также то, что выбор терапии проводился по усмотрению врача, не позволяют убедительно подтвердить эффективность применения RBV у этих больных. Из вышесказанного следует, что применение комбинации SOF + DCV с RBV в течение 12 нед. можно рекомендовать пациентам, инфицированным HCV генотипа 1, с декомпенсированным циррозом печени стадии B по шкале Чайлда-Пью. Необходимы дополнительные данные относительно пациентов с более тяжелым поражением печени (стадия C по шкале Чайлда-Пью).
Sofosbuvir and Simeperevir
The effectiveness of the SOF + SMV scheme without RBV for 12 weeks. It was studied in a clinical study of the III phase, which was attended by patients infected with HCV genotype 1, with compensated cirrhosis of the liver (density defined by the Fibroscan method, more than 12.5 kPa). The IVV frequency was lower than expected: 88 (44 of 50), 79 (42 out of 53), 83 (60 out of 72) and 84% (26 of 31) in patients who had previously received treatment already received therapy, patients infected with HCV genotypes 1a and 1b, respectively. Unfortunately, the effectiveness of the SOF + SMV scheme with RBV, prescribed depending on the body weight, for 12 weeks. This study did not estimate. The data obtained when using other combinations with SOF without IFN indicate that the addition of RBV appointed depending on body weight (1000 or 1200 mg in patients with body weight< 75 и? 75 кг соответственно), к SOF и SMV можно рекомендовать у пациентов с компенсированным циррозом, инфицированных HCV генотипа 1. Эффективность и безопасность применения SOF + SMV в течение 12 или 24 нед. с RBV или без него у больных с декомпенсированным циррозом, инфицированных HCV генотипа 1, оценивались в нескольких реальных когортах . Результаты этих исследований свидетельствуют о том, что добавление RBV может повысить частоту УВО12 в этой популяции .
Paritaprevir-based schemes
In large randomized clinical studies of the III phase, the effectiveness and safety of the 3-PPT scheme with RBV (1000 or 1200 mg / day, depending on the body weight) used for 12 or 24 weeks, was studied. In 380 infected HCV genotype 1 patients with compensated cirrhosis of the liver (score from Metavir\u003e F3, or on the ISHAK\u003e 4 scale, or FIBROSCAN results? 14.6 kPa). In analyzes in subgroups, it was found that the difference in the frequency of UVV12 between subgroups that received therapy for 12 and 24 weeks was due to a predominantly distinguished response in patients with 1a genotype under the previous response to treatment. These data are confirmed by the fact that both the virus subtype and the absence of an answer to previous therapy were determined as predictors of UVV12. Patients with cirrhosis of the liver, who did not have previously answered the therapy, reached UVV12 in 86.7 and 95.2% of cases during treatment for 12 and 24 weeks. respectively. Thus, in patients with genotype 1a, under the earlier response to treatment, the frequency of UVO12 was 80% (40 of 50) in treatment for 12 weeks. and 93% (39 of 42) in the treatment within 24 weeks. In all other subgroups of patients with genotype 1a, including patients who did not receive previously obtained treatment, as well as patients with partial response and relapse after preceding therapy, the response rate ranged from 92 to 100% in treatment for 12 and 24 weeks. Among patients with genotype 1B, all patients, except for one, reached UVV12 in the treatment for both 12 and 24 weeks. . Considering these data, as well as the results obtained in patients without a liver cirrhosis (see Table 2), it is obvious that the need to evaluate the effectiveness of the scheme without RBV in patients infected with HCV genotype 1A is absent. Nevertheless, the role of RBV and the need to include it for maximum increase in the frequency of response in patients infected with HCV genotype 1b, with compensated liver cirrhosis remained not fully established in this clinical study. In this regard, the effectiveness of the application of 3-PPAP scheme without RBV in this population of patients was evaluated. UVO12 was achieved in all 60 patients infected with HCV genotype 1b, with compensated cirrhosis (Score from Metavir\u003e F3, or on the ISHAK\u003e 4 scale, or FIBROSCAN results? 12.5 kPa), including previously treated treatment or previously therapy Pegifn and RBV patients. This indicates the absence of the need to add RBV in these patients (see Table 2).

Daclatasvir-based schemes
The effectiveness of the combination of DCV + SMV with RBV or without it was studied in patients with liver cirrhosis infected with HCV genotype 1b. Its use was accompanied by a smaller frequency of UVO12 (69.2%) compared with patients without cirrhosis (82.6%). However, a small number of patients with cirrhosis could be the cause of the variability of the results different patients. The effect of RBV on the effectiveness of therapy in patients with cirrhosis in the present study was not subject to analysis due to their small number.
In patients infected with HCV genotype 1, with compensated cirrhosis of the liver (score from the Metavir F4 scale, or Fibroscan results? 14,6 kPa, or Fibrotest? 0.75 and apri\u003e 2) after 12 weeks. Applications 3-PPPs with fixed doses DCV, ASV, Beklabuvir with RBV (1000-1200 mg / day) or without it The total frequency of UVO12 amounted to 93%. In patients infected with HCV genotype 1A, when adding RBV, this figure was 7% higher in patients who did not receive previously treated, and by 5% in patients who have previously received therapy. On the contrary, RBV did not affect the achievement of response in patients with HCV genotype 1b; In general, 51 of 52 patients infected with HCV genotype 1b reached UVV12. Despite the fact that the difference in achieving UVV12 associated with the use of RBV, in patients infected with HCV genotype 1a, was moderate, it suggests that the inclusion of RBV can increase the effectiveness of therapy in patients with liver cirrhosis. The role of RBV is more complicated, since the study did not have sufficient power for the statistical assessment of the RBV contribution to the outcomes of efficiency. Today, the development of this combination is discontinued. Thus, diagrams based on DCV with RBV or without it will not be used in patients with cirrhosis of the liver infected with HCV genotype 1.
The effect of RBV on the effectiveness of therapy in patients infected with HCV genotypes 2, 3 and 4
SophosBuvir-based schemes
Genotype 2.
In 4 studies of the III phase, it was shown that when using a combination of SOF + RBV (1000 or 1200 mg in patients with body weight< 75 и? 75 кг соответственно) в течение 12 нед. частота УВО превышает 90 % у большинства пациентов, инфицированных HCV генотипа 2. Исключение составляют больные с циррозом печени, уже получавшие ранее лечение, у которых, по-видимому, эффективна более продолжительная терапия. У этих больных частота УВО12 после 12 и 16 нед. лечения SOF + RBV составила 60 (6 из 10) и 78 % (7 из 9) соответственно . Позднее в другом исследовании частота УВО12 равнялась 87 (13 из 15) и 100 % (17 из 17) после 16 и 24 нед. соответственно . Эти результаты свидетельствуют о том, что терапия по схеме SOF + RBV (назначаемым в зависимости от массы тела) является стандартным методом лечения для всех пациентов, инфицированных HCV генотипа 2, за исключением больных с циррозом печени, у которых продолжительность лечения рекомендуется увеличить до 24 нед.
GENOTIP 3.
In patients infected with HCV genotype 3, the IVV frequency was lower than in patients with HCV genotype 2. A more pronounced effect was found in them with an increase in the length of the therapy Sof + RbV (1000 or 1200 mg in patients with body weight increase< 75 и? 75 кг соответственно) до 24 нед. Частота УВО у пациентов, инфицированных HCV генотипа 3, варьировала в зависимости от проведения и эффективности предшествовавшей терапии и наличия цирроза печени (на основании результатов биопсии печени, или результатов FibroScan > 12.5 kPa, or fibrotest\u003e 0.75 and apri\u003e 2). Among patients who have not received previously treated treatment, the frequency of UVO12 amounted to 92% in patients with cirrhosis and 95% without it. However, among those who have previously received treatment with HCV genotype 3, the frequency of WEVO was lower: 62% in patients with cirrhosis and 87% in patients without a liver cirrhosis. Thus, in the future, it requires a search for more efficient combinations and an assessment of the effect on the effectiveness of treatment in patients infected with HCV genotype 3.
The effectiveness of the combination of SOF with an NS5A and RBV inhibitor (1000 or 1200 mg / day depending on body weight) or without it was estimated in several open studies. When using a combination of Sof + DCV with RBV or without it within 24 weeks. UVV12 has reached a total of 89% of 18 patients without liver cirrhosis infected with HCV genotype 3. It is more interesting that the use of a combination of Sof + DCV without RBV for 12 weeks. It was estimated in 152 infected HCV genotype 3 patients who have not received and have previously received treatment, without cirrhosis and with compensated cirrhosis (Metavir F4, or Fibroscan\u003e 14.6 kPa, or Fibrotest? 0.75 and APRI\u003e 2). The frequency of UVV12 amounted to 97 (73 of 75) and 94% (32 of 34) in patients without liver cirrhosis that have not received and have previously received treatment, respectively. However, in patients with liver cirrhosis (63%), this indicator was lower: 58 (11 out of 19) and 69% (9 out of 13) in patients who have not received and have previously received treatment, respectively. In an uncontrolled cohort study in real clinical practice, the effectiveness of therapy according to the SOF + DCV scheme for 12 weeks was confirmed. In patients infected with HCV genotype 3, without severe liver fibrosis. These results suggest that in patients with HCV genotype 3 without cirrhosis, the SOF + DCV scheme can be applied for 12 weeks. without RBV. On the contrary, it is necessary to estimate the potential positive effect of RBV in patients with liver cirrhosis. In patients with decompensated cirrhosis of the liver, included in the program for increasing the availability of medical care, the frequency of UVO12 was similar to those receiving Sof + DCV with RBV and without it (70 and 71%, respectively). Nevertheless, it is impossible to make certain conclusions on the basis of the results obtained in this cohort (the addition of RBV was performed at the discretion of the attending physician, and only 7 patients were included in the group without RBV). The effectiveness of using the combination of Sof + DCV with RBV (prescribed depending on body weight) and without it for 12 and 16 weeks. Currently, it is studied in patients infected with HCV genotype 3, with severe fibrosis or compensated cirrhosis (ClinicalTRials.gov, No. NTC02319031). Optimization of treatment outcomes in patients with cirrhosis of the liver may include an increase in the duration of treatment (up to 24 weeks) with the addition of RBV or without it. The preliminary data obtained in a real uncontrolled cohort seems to indicate an increase in treatment efficacy (uvo4 88%) in patients with cirrhosis with an increase in the duration of treatment up to 24 weeks. Currently, it is impossible to estimate the potential role of RBV in this population with such a duration of treatment. The optimal scheme combining the use of SOF + DCV and the need to add RBV in patients with cirrhosis of the liver infected with HCV genotype 3 are subject to further study.
The effectiveness of the use of the combination Sof + LDV with RBV and without it for 12 weeks. It was estimated in 51 patients infected with HCV genotype 3, not previously obtained treatment. The higher frequency of UVO12 was observed in patients receiving RBV compared with patients in which RBV was not added to the treatment regimen (100 VS 64%, respectively). Nevertheless, it was found that the presence of a cirrhosis can reduce the frequency of WEV in patients with HCV genotype 3 receiving Sof + LDV with RBV for 12 weeks. Thus, the frequency of UVO12 amounted to 73% in 22 treatment of patients with cirrhosis compared with 89% in 28 patients who had previously obtained patients without a liver cirrhosis. The effectiveness of the SOF + LDV circuit for 12 weeks. Increased by adding RBV in patients with decompensated cirrhosis, but remained significantly lower than the effectiveness of the SOF + DCV scheme with RBV or without it. In the same way, the addition of RBV increased the frequency of UVO12 in the HCV of the HCV genotype 3 of the previously treated patients with cirrhosis treated with therapy according to the SOF + GS-5816 scheme (second-generation inhibitor) for 12 weeks. (88 VS 96%). Based on the above, the use of RBV, apparently, is mandatory in patients with cirrhosis of the liver infected with HCV genotype 3 receiving a short course of therapy with a combination of PPPD.
Genotype 4.
In an open study, which was attended by 21 patients infected with HCV genotype 4, with cirrhosis and without it, which did not receive and previously obtained treatment, the frequency of UVO12 was 95% after 12 weeks. Therapies according to SOF + LDV scheme. This, apparently, indicates the absence of the need to add RBV in this group of patients. Nevertheless, to make certain conclusions, the presence of additional results obtained in clinical studies and real cohorts is required. When combining outputs with data obtained in patients infected with HCV genotype 1, the RBV role estimate remains necessary in the SOF + LDV scheme, especially in patients with cirrhosis infected with HCV genotype 4.
Paritaprevir / Ritonavir and Obitasvir (Scheme 2-PPTD) are also characterized by an antiviral effect against HCV genotype 4. The effectiveness of the application of the circuit 2-PPAP with RBV (depending on the body weight) or without it for 12 weeks. It was studied in a phase II study, which was attended by patients infected with HCV genotype 4, which did not have cirrhosis and not previously received treatment. UVV12 was achieved by all patients obtained by RBV (42 of 42), and 90.9% of patients (40 of 44), which have not been added RBV. The failures were mainly due to virological reasons (1 - breakthrough, 2 - recurrences and 1 - disposal from under observation), indicating that RBV increases the likelihood of achieving WSV in this population. Taking into account this data, the 2-PPT scheme with RBV (depending on body weight) for 12 weeks. Used in patients without cirrhosis infected with HCV genotype 4, which have previously received therapy. All patients (42 of 42) reached UVV12, which indicates that the 2-PPT scheme with RBV for 12 weeks. It is the optimal method of treating all patients without cirrhosis of the liver infected with HCV genotype 4. Currently, the effectiveness of the 2-PPAP circuit with RBV in patients with compensated cirrhosis is carried out (clinicaltrials.gov, No. NCT02265237).
Effect of RBV for the safety of treatment
In tab. 3 summarized the most frequent undesirable phenomena arising against the background of the use of SOF / LDV for 12 weeks. With the addition of RBV (1000 or 1200 mg / day, depending on the body weight) or without it. Adding RBV led to risk of fatigue, insomnia, irritability and anemia. Nevertheless, there were no severe cases of anemia (hemoglobin less than 85 g / l). The anemia easily was adjusted by reducing the dose of RBV without affecting the achievement of UVV. The Sirius study was designed in such a way that the possibility of an informal comparison of the frequency of unwanted phenomena between patients with liver cirrhosis, receiving placebo, Sof + LDV + RBV (depending on body weight) and Sof + LDV. In general, the frequency of unwanted phenomena was high (\u003e 80%) and similar in all three groups. In the Sof + LDV + RBV group, the headache frequency was lower than in the placebo group, and the fatigue frequency was lower than in the SOF + LDV group. Most pathological changes in laboratory indicators of III-IV degree noted against the background of the application of placebo. In 1 (1%) of the patient developed anemia (hemoglobin less than 85 g / l) during the period of active treatment, which required blood transfusions. None of the patients were appointed to the ErythropoEZ funds. On the other hand, the combined results 3 of clinical studies of the III phase indicate that the application of SOF + LDV-based scheme leads to improving the quality of life and improve other outcomes measured by patients, regardless of the lesion stage of the liver and that the most significant reduction in the quality of life has been due using RBV. In general, the addition of RBV appointed depending on body weight, to a scheme containing a sofosbuvir, in patients with liver cirrhosis safely and is well tolerated.

In tab. 4 shows unwanted phenomena, most often arising against the background of the application of 3-PPP scheme. In most patients, at least one undesirable phenomenon developed, however, in most cases, these phenomena were easy severity. The frequency of severe undesirable phenomena and phenomena, which caused the discontinuation of treatment, in the studies were low, but at the same time numerically higher in patients with liver cirrhosis. Unwanted phenomena arising in 5% of cases or less when using a 3-PPD and RBV scheme (depending on body weight) compared with placebo, were regarded as associated with the use of antiviral drugs. These phenomena were fatigue, nausea, itching, insomnia, asthenia and anemia. The frequency of these undesirable phenomena was, as a rule, below in a group that did not receive RBV. In general, the frequency of unwanted phenomena in patients with cirrhosis and without cirrhosis was similar. The transient increase in total bilirubin (mainly due to indirect) was due to the suppression of the OATP1B1 parachoprem (organic anions transport polypeptide 1B1) and OATPB3 (organic anions transport polypeptide 1B3), as well as RBV-induced hemolysis. Hyperbilirubinemia was less common in patients treated according to a 3-PPT scheme without RBV, compared with patients who have RBV added to this scheme, which suggests that it has been associated with the use of RBV. Anemia II degree (hemoglobin less than 100 g / l) was registered in 6% of patients without liver cirrhosis received by treatment according to 3-PDAPs with RBV for 12 weeks, and 7 and 11% of patients with cirrhosis treated according to the scheme 3-PPT for 12 and 24 weeks. accordingly. Anemia III degree (hemoglobin less than 80 g / l) has rarely developed. The reduction in the level of hemoglobin was adjusted mainly by reducing the RBV dose, which was not reflected in the achievement of uvo. Cases of anemia registered during clinical studies were mainly regarded as associated with the use of RBV, since when using a 3-PPAP scheme without RBV, anemia was not observed.

RBV application: risk and benefit ratio
The decision to add RBV should be taken for each patient separately, taking into account the risk and benefit ratio: some increase in efficiency and reduce the duration of the VS treatment deterioration of the safety and quality profile, due to the development of anemia. Most patients receive excessive treatment due to the addition of RBV, because it is impossible to select on the basis of various initial data of patients who absolutely need to use this drug. A certain role can play the severity of liver damage. It is also possible to communicate between the results of the FibroScan test and the effectiveness of treatment. Another factor may be the initial presence of viral strains resistant to NS5A inhibitors. In patients with cirrhosis received treatment according to SOF + LDV scheme, it was found that in the presence of such options, the addition of RBV allowed to achieve a higher frequency of WEVV than in treating without RBV, but in the absence of these options, WSV indicators on the RBV background were the same, how without it. Unfortunately, the study of resistance cannot be implemented and recommended to all patients with liver cirrhosis. One method of improving the risk and benefit ratio may be a more thorough definition of the optimal Dose of RBV when it is combined with 3-PPT. As a rule, in this case, the RBV dose is used, calculated for use in the PEGIFN + RBV scheme. The use of a scheme containing SOF, or a circuit with 2-PPPs or 3-PPPs with low doses RBV (600 or 800 mg per day), may increase the frequency of WEV compared to the schemes without RBV. At the same time, the frequency of toxic phenomena associated with the use of RBV (assigned depending on body weight) will be minimized. In practice, it is recommended to begin treatment with the assignment of RBV in accordance with the body weight, and then adjust the dose of the drug, taking into account the level of hemoglobin and kidney function. Finally, the use of RBV is problematic in a number of groups, such as patients on hemodialysis, as well as patients who are planned or organized transplantation. Under these conditions, an individual approach to the choice of dose of the drug is required. A deeper understanding of the mechanism of action of the drug can provide the electoral use of RBV in the ERU of PPPD.
Conclusion
Modern fully oral treatment regimens that do not contain IFN make it possible to achieve an IVO in more than 90% of cases, as well as reduce the duration of treatment in most patients with CGC, including patients with liver cirrhosis and have previously received therapy. This fact, along with a more favorable security profile, helps to increase the effectiveness of treatment compared to IFN-based schemes. There are many PPP combinations with which you can achieve an optimal ratio of efficiency and security of therapy. Each these schemes can be modified by various parameters, including the use of RBV. In tab. 5 shows the indications for adding RBV to the main schemes in accordance with the characteristics of patients and the virus. When using combinations based on SOF, the use of RBV is advisable in the following situations: in patients infected with HCV genotype 1, which have previously obtained treatment and having cirrhosis or decompensated cirrhosis of the liver, and in patients infected with HCV genotype 3, with cirrhosis of the liver. As in many similar situations, the difference was not statistically significant for patients with HCV genotype 1, and the question of whether RBV in patients with HCV genotype 3 with cirrhosis receiving Sof + DCV still requires studying. In these situations, adding RBV reduces the duration of treatment to 12 weeks. In most cases, leading to a decrease in its value. It is necessary to find out the need to use RBV in patients with cirrhosis of the liver, receiving the treatment of SOF and SMV. The inclusion of RBV is recommended in the treatment of all patients infected with HCV genotypes 1a and 4 receiving 3-PDAP combinations and 2-PPDs, respectively. Since RBV is an inexpensive drug that is well tolerated during a combination with IFN schemes, it remains an effective means for improving the CGS therapy schemes and optimizing the results of their application.
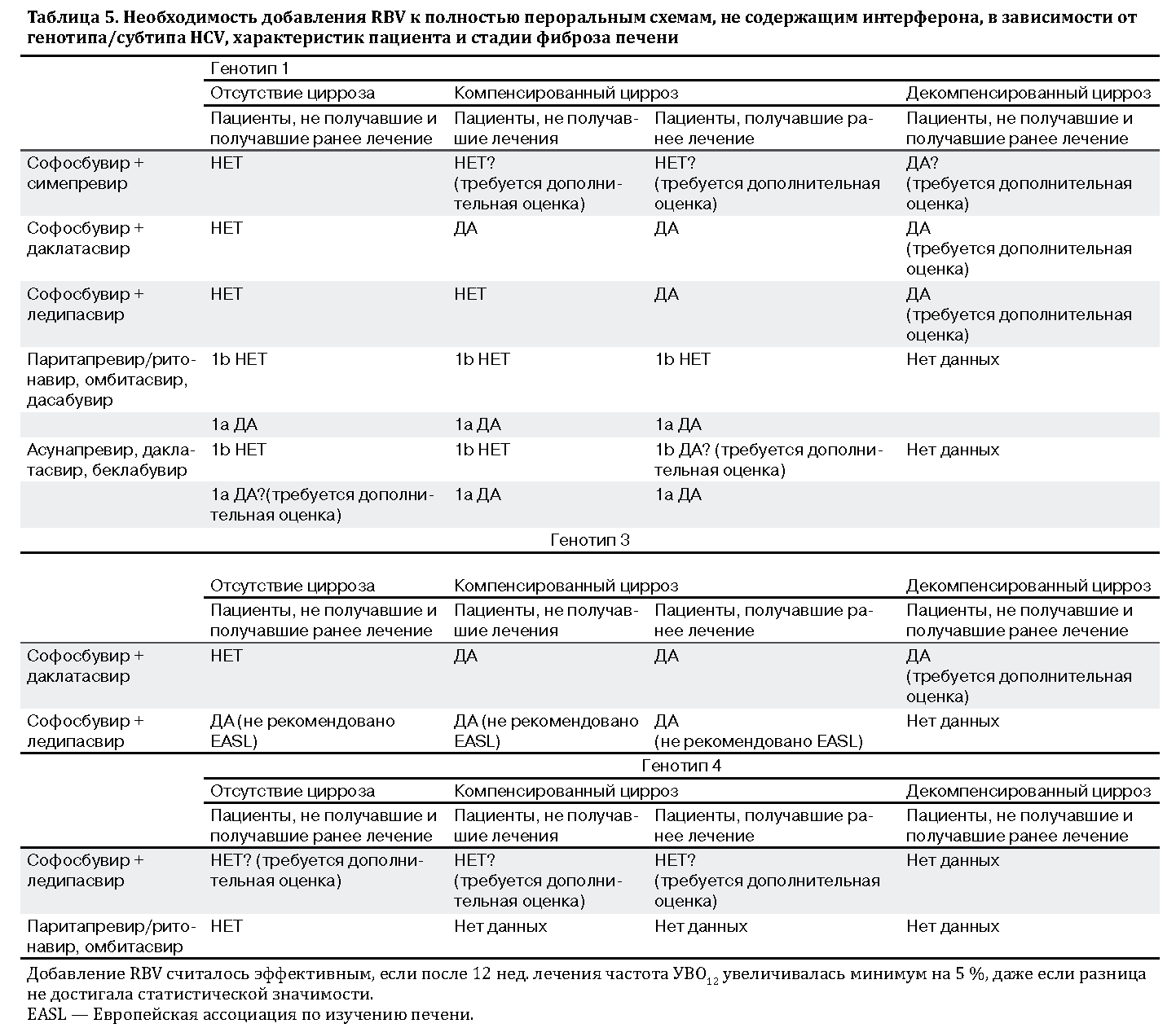
Conflicts of interest
Hezode worked as a speaker and consultant in ABBVIE, Bristol-Myers Squibb, Gilead Sciences, Janssen Pharmaceuticals, Merck Sharp & Dohme and Roche.
Jean-Pierre Bronowicki worked as a clinical researcher, speaker and / or consultant in companies Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, JanSsen Pharmaceuticals, Merck Sharp & Dohme, Novartis and Roche.
Contribution authors
Literature
- WORLD HEALTH ORGANIZATION. Hepatitis C Key Facts. WHO FACTSHEET NO 164, 2013.
- MOHD HANAFIAH K, GROEGER J, FLAXMAN AD, WIERSMA ST. Global Epidemiology of Hepatitis C Virus Infection: New Estimates of Age-Specific Antibody to HCV Seroprevalence. Hepatology 2013; 57: 1333-1342.
- Smith DB, Bukh J, Kuiken C, Muerhoff As, Rice CM, Stapleton JT, et al. Expanded Classification of Hepatitis C Virus INTO 7 GENOTYPES AND 67 SUNOTYPES: UPDATED CRITERIA AND GENOTYPE ASSIGNMENT WEB RESOURCE. Hepatology 2014; 59: 318-327.
- American Association For the Study of Liver Diseases, Infectious Diseases Society of America. Recommendations for Testing, Managing, And Treating Hepatitis C. Available AT
- European Association for the Study of the Liver. Easl Clinical Practice Guidelines: Management of Hepatitis C Virus Infection. J Hepatol 2014; 60: 392-420.
- Bronowicki JP, Ouzan D, Asselah T, Desmorat H, Zarski JP, Foucher J, et al. Effect of Ribavirin In Genotype 1 Patients with Hepatitis C Responding to Pegylated Interferon Alfa-2a Plus Ribavirin. Gastroenterology 2006; 131: 1040-1048.
- Hezode C, Forestier N, Dusheiko G, Ferenci P, POL S, GOESER T, ET Al. Telaprevir and Peginterferon with or Without Ribavirin for Chronic HCV Infection. N ENGL J MED 2009; 360: 1839-1850.
- Kowdley KV, Lawitz E, Poordad F, COHEN DE, Nelson Dr, Zeuzem S, et al. Phase 2B Trial Of Interferon-Free Therapy for Hepatitis C Virus Genotype 1. N ENGL J MED 2014; 370: 222-232.
- Lawitz E, PoORDAD FF, Pang PS, Hyland Rh, Ding X, MO H, et al. Sofosbuvir and Ledipasvir Fixed-Dose Combination With and Previously Treated PatientNaive And Previously Treated Patients with Genotype 1 Hepatitis C Virus Infection (Lonestar): An Open-Label, Randomised, Phase 2 Trial. Lancet 2014; 383: 870.
- Pawlotsky Jm, Dahari H, Neumann Au, Hezode C, Germanidis G, Lonjon I, et al. AntiRial Action of Ribavirin In Chronic Hepatitis C. Gastroenterology 2004; 126: 703-714.
- Thomas E, Ghany Mg, Liang TJ. The Application and Mechanism of Action Of Ribavirin In Therapy Of Hepatitis C. Antivir Chem Chemother 2012; 23: 1-12.
- Dietz J, Schelhorn SE, Fitting D, Mihm U, Susser S, Welker MW, et al. Deep Sequencing Reveals Mutagenic Effects of Ribavirin During Monotherapy of Hepatitis C Virus Genotype 1-Infected Patients. J Virol 2013; 87: 6172-6181.
- Mihm U, Welker MW, Teuber G, Wedemeyer H, Berg T, Sarrazin C, et al. Impact of Ribavirin Priming On Viral Kinetics and Treatment Response in Chronic Hepatitis C Genotype 1 INFECTION. J VIRAL HEPAT 2014; 21: 42-52.
- Rotman Y, Noureddin M, Feld JJ, Guedj j, WitThaus M, Han H, et al. Effect of Ribavirin On Viral Kinetics and Liver Gene Expression In Chronic Hepatitis C. Gut 2014; 63: 161-169.
- Hezode C, Bouvier-Alias \u200b\u200bM, Costentin C, Medkour F, Franc-Poole E, Alyson M, et al. Effect of An Impdh Inhibitor, Merimepodib (MMPD), ASSESSED ALONE OR IN COMBINATION WITH RIBAVIRATION, ON HCV REPLICATION: Implications Regarding Ribavirin's Mechanisms of Action. Hepatology 2006; 44: 615A.
- Gane EJ, STEDMAN CA, HYLAND RH, Ding X, Svarovskaia E, Symonds WT, et al. Nucleotide Polymerase Inhibitor Sofosbuvir Plus Ribavirin for Hepatitis C. N ENGL J MED 2013; 368: 34-44.
- Osinusi A, Meissner EG, Lee YJ, Bon D, Heytens L, Nelson A, et al. Sofosbuvir and Ribavirin for Hepatitis C GENOTYPE 1 IN PATIENTS WITH UNFAVORABLE TREATMIISTICS: A RANDOMIZED CLINICAL TRIAL. Jama 2013; 310: 804-811.
- Kowdley KV, Gordon SC, Reddy Kr, Rossaro L, BERNSTEIN DE, Lawitz E, et al. Ledipasvir and Sofosbuvir for 8 or 12 Weeks for Chronic HCV WITHOUT CIRRHOSIS N ENGL J MED 2014; 370: 1879-1888.
- AFDHAL N, ZEUZEM S, KWO P, CHOJKIER M, GITLIN N, PUOTI M, ET AL. Ledipasvir and Sofosbuvir for Untreated HCV Genotype 1 INFECTION. N ENGL J MED 2014; 370: 1889-1898.
- AFDHAL N, REDDY KR, NELSON DR, LAWITZ E, GORDON SC, SCHIFF E, ET AL. Ledipasvir and Sofosbuvir for Previously Treated HCV Genotype 1 Infection. N ENGL J MED 2014; 370: 1483-1493.
- GAO M. AntiRial Activity and Resistance of HCV NS5A Replication Complex Inhibitors. Curr Opin Virol 2013; 3: 514-520.
- Sulkowski MS, Gardiner DF, Rodriguez-Torres M, Reddy Kr, Hassanein T, Jacobson I, et al. Daclatasvir Plus Sofosbuvir for Previously Treated or Untreated Chronic HCV Infection. N ENGL J MED 2014; 370: 211-221.
- POL S, Bourliere M, Lucier S, De Ledinghen V, Zoulim F, Dorival-Mouly C, et al. Safety and Efficacy of the Combination Daclatasvir-Sofosbuvir in HCV Genotype 1-Mono-Infected Patients from The Frenc Observational Cohort Anrs C022 Hepather. J Hepatol 2015; 62: S258.
- Lawitz E, Sulkowski MS, Ghalib R, Rodriguez-Torres M, Younossi ZM, Corregidor A, et al. SIMEPREVIR PLUS SOFOSBUVIR, WITH OR WITHOUT RIBAVIRIN, TO TREAT CHRONIC INFECTION WITH HEPATITIS C VIRUS GENOTYPE 1 IN NON-RIBONDERS TO PEGYLATED INTERFERON AND RIBAVIRIN AND TREATMENT-NAIVE PATIENTS: THE COSMOS RANDOMISED STUDY. Lancet 2014; 384: 1756-1765.
- KWO P, Gitlin N, NaSSS R, Berstein D, Rojter S, Schiff E, et al. A Phase 3, Randomised, Open-Label Study to Evaluate The Efficacy and Safety of 8 and 12 Weeks of Simeprevir (SMV) Plus Sofosbuvir (Sof) in Treatment-Naive and -Experiened Patients with Chronic HCV Genotype 1 INFECTION WITHOT CIRRHOSIS: OPTIMIST- one. J Hepatol 2015; 62: S270.
- Feld JJ, Kowdley KV, Coakley E, Sigal S, Nelson Dr, Crawford D, et al. Treatment of HCV WITH ABT-450 / R-OMBITASVIR AND DASABUVIR WITH RIBAVIRIN. N ENGL J MED 2014; 370: 1594-1603.
- Ferenci P, BERNSTEIN D, Lalezari J, Cohen D, Luo Y, Cooper C, et al. ABT-450 / ROMBITASVIR AND DASABUVIR WITH OR WITHOUT RIBAVIRIN FOR HCV. N ENGL J MED 2014; 370: 1983-1992.
- Zeuzem S, Jacobson IM, Baykal T, Marinho RT, Poordad F, Bourliere M, et al. Retreatment of HCV WITH ABT-450 / R-OMBITASVIR AND DASABUVIR WITH RIBAVIRIN. N ENGL J MED 2014; 370: 1604-1614.
- Andreone P, Colombo MG, Enejosa JV, Koksai I, Ferenci P, Maieron A, et al. ABT-450, Ritonavir, OMBITASVIR, and Dasabuvir Achieves 97% and 100% Sustained Virologic Response with or Without Ribavirin in Treatment-Experiated Patients with HCV GENOTYPE 1B INFECTION. Gastroenterology 2014; 147: 359-365.
- Zeuzem S, Hezode C, Bronowicki JP, Loustaud-Ratti V, GEA F, Buti M, et al. Daclatasvir Plus Simeprevir with or Without Ribavirin for The Treatment of Chronic Hepatitis C Virus Genotype 1 INFECTION. J Hepatol 2015. http://dx.doi.org/10.1016/j.jhep.2015.09.024 ,.
- McPhee F, Sheaffer AK, FRIBORG J, Hernandez D, Falk P, Zhai G, et al. Preclinical Profile and Characterization of the Hepatitis C Virus NS3 Protease Inhibitor Asunaprevir (BMS-650032). Antimicrob Agents Chemother 2012; 56: 5387-5396.
- Lok As, Gardiner DF, Lawitz E, Martorell C, Everson GT, Ghalib R, et al. PRELIMINARY STUDY OF TWO ANTIVIRAL AGENTS FOR HEPATITIS C GENOTYPE 1. N ENGL J MED 2012; 366: 216-224.
- Manns M, Pol S, Jacobson Im, Marcellin P, Gordon SC, Peng Cy, et al. All-Oral Daclatasvir Plus Asunaprevir for Hepatitis C Virus Genotype 1B: A Multinational, Phase 3, Multicohort Study. Lancet 2014; 384: 1597-1605.
- Jensen D, Sherman Ke, Hezode C, POL S, Zeuzem S, De Ledinghen V, et al. Daclatasvir and Asunaprevir Plus Peginterferon Alfa and Ribavirin in HCV Genotype 1 and 4 non-responders. J Hepatol 2015; 63: 30-37.
- EVERSON GT, SIMS KD, RODRIGUEZ-TORRES M, Hezode C, Lawitz E, Bourliere M, et al. Efficacy of An Interferon- and Ribavirin-Free Regimen of Daclatasvir, AsunaPrevir, and BMS-791325 in Treatment-Naive Patients with HCV GENOTYPE 1 INFECTION. Gastroenterology 2014; 146: 420-429.
- PoORDAD F, SIEVERT W, Mollisson L, Bennett M, Tse E, Brau N, et al. Fixed-Dose Combination Theraprevir, and Beclabuvir for noncirrhotic Patients with HCV GENOTYPE 1 INFECTION. Jama 2015; 313: 1728-1735.
- Reddy KR, Bourliere M, Sulkowski M, Omata M, Zeuzem S, Feld JJ, et al. Ledipasvir and Sofosbuvir in Patients with Genotype 1 Hepatitis C Virus Infection and Compensated Cirrhosis: An Integrated Safety and Efficacy Analysis. Hepatology 2015; 62: 79-86.
- Bourliere M, Bronowicki J-P, De Ledinghen V, Hezode C, Zoulim F, Mathurin P, et al. LEDIPASVIR AND SOFOSBUVIR FOR 12 WEEKS ALONE IN PATIENTS WITH GENOTYPE 1 HCV INFECTION AND CIRRHOSIS IN WHM PRIOR PROTEASE INHIBITOR THERAPY FAILED (Sirius): a randomized, Double-Blind, Phase 2 Trial. Lancet Infect DIS 2015; 15: 397-404.
- Gane EJ, Hyland Rh, An D, Pang PS, Symonds WT, Mchutchison JG, et al. Sofosbuvir / LedispaSvir Fixed Dose Combination Is Safe and Effective in DiffiCult-to-Treat Populations Including Genotype-3 Patients, DecoMpenSated Genotype-1 Patients, and Genotype-1 Patients with Prior Sofosbuvir Treatment Experience. J Hepatol 2014; 60: S3-S4.
- CHARLTON M, EVERSON GT, FLAMM SL, KUMAR P, LANDIS C, BROWN JR RS, ET AL. Ledipasvir and Sofosbuvir Plus Ribavirin for Treatment of HCV INFECTION IN PATIENTS WITH ADVANCED LIVER DISEASE. Gastroenterology 2015; 149: 649-659.
- Foster G, McLauchlan J, Irving W, Cheung M, Hudson B, Verna S, et al. Treatment of DecoMPensated HCV Cirrhosis in Patients with Diverse Genotypes: 12 Weeks Sofosbuvir and NS5A Inhibitors WITH / WITHOUT RIBAVIRIN IS EFFECTIVE IN HCV GENOTYPES 1 AND 3. J HEPATOL 2015; 62: S190.
- PoORDAD F, SCHIFF ER, VIERLING JM, LANDIS C, FONTANA RJ, YANG R, ET AL. Daclatasvir, Sofosbuvir and Ribavirin Combination for HCV Patients with Advanced Cirrhosis or PostTransplant Recurrence: Phase 3 Ally-1 Study. J Hepatol 2015; 62: S261.
- Lawitz E, Matusow G, Dejesus E, Yoshida E, Felizarta F, Ghalib R, et al. A Phase 3, Open-Label, Single Arm Study to Evaluate The Efficacy and Safety of 12 Weeks of Simeprevir (SMV) Plus Sofosbuvir (SOF) in Treatment-Naive or -Experiened Patients with Chronic HCV GENOTYPE 1 INFECTION AND CIRRHOSIS: OPTIMIST-2 . J Hepatol 2015; 62: S264.
- Modi AA, Nazario H, Trotter JF, Gautam M, Weinstein J, Mantry P, et al. Safety and Efficacy of Simeprevir Plus Sofosbuvir with or Without Ribavirin In Patients 1 Hepatitis C Cirrhosis. Liver Transpl 2015. http://dx.doi.org/10.1002/LT.24324 ,.
- SAXENA V, NYBERG L, PAULY M, DASGUPTA A, NYBERG A, PIASECKI B, ET AL. Safety and Efficacy of Simeprevir / Sofosbuvir in Hepatitis C-Infected Patients with Compensated and Decompensated Cirrhosis. Hepatology 2015; 62: 715-725.
- AQEL BA, PUNGPAPONG S, LEISE M, WERNER KT, CERVENAK AE, WATT KD, ET AL. Multicenter Experience using Sixout Ribavirin to Treat Hepatitis C GENOTYPE 1 IN PATIENTS WITH CIRRHOSIS. Hepatology 2015; 62: 1004-1012.
- PoORDAD F, HEZODE C, TRINH R, KOWDLEY KV, Zeuzem S, Agarwal K, et al. ABT-450 / R-OMBITASVIR AND DASABUVIR WITH RIBAVIRIN FOR HEPATITIS C WITH CIRRHOSIS. N ENGL J MED 2014; 370: 1973-1982.
- Feld JJ, Moreno C, Trinh R, Tam E, Bourgeois S, Horsmans Y, et al. Sustained Virologic Response of 100% in HCV GENOTYPE 1B PATIENTS WITH CIRRHOSIS RECEIVING OMBITASVIR / PARITAPREVIR / R AND DASABUVIR FOR 12 WEEKS. J Hepatol 2015. http://dx.doi.org/10.1016/j.jhep.2015.10.005 ,.
- Muir AJ, Poordad F, Lalezari J, Everson G, Dore GJ, Herring R, et al. Daclatasvir in combination with asunaprevir and baclabuvir for hepatitis C Virus Genotype 1 INFECTION WITH COMPENSATED CIRRHOSIS. JAMA 2015; 313: 1736-1744.
- Jacobson IM, Gordon SC, Kowdley KV, Yoshida Em, Rodriguez-Torres M, Sulkowski MS, et al. Sofosbuvir for Hepatitis C Genotype 2 OR 3 in Patients WITHOUT TREATMENT OPTIONS N ENGL J MED 2013; 368: 1867-1877.
- Lawitz E, Mangia A, Wyles D, Rodriguez-Torres M, Hassanein T, Gordon SC, et al. Sofosbuvir for Previous Untreated Chronic Hepatitis C INFECTION. N ENGL J MED 2013; 368: 1878-1887.
- Zeuzem S, Gm Dusheiko, Salupere R, Mangia A, Flisiak R, Hyland Rh, et al. Sofosbuvir and Ribavirin In HCV GENOTYPES 2 AND 3. N ENGL J MED 2014; 370: 1993-2001.
- Foster GR, Pianko S, Brown A, Forton D, NaSSS RG, George J, et al. Efficacy of Sofosbuvir Plus Ribavirin WITH OR WITHOUT PEGINTERFERON-ALFA IN PATIENTS WITH HCV GENOTYPE 3 INFECTION AND TREATMENT-EXPERIENCED PATIENTS WITH CIRRHOSIS AND HCV GENOTYPE 2 INFECTION. Gastroenterology 2015. http://dx.doi.org/ 10.1053 / j.gastro.2015.07.043,.
- Nelson Dr, Cooper JN, Lalezari JP, Lawitz E, Pockros PJ, Gitlin N, et al. All-Oral 12-Week Treatment with Daclatasvir Plus Sofosbuvir in Patients with Hepatitis C Virus Genotype 3 INFECTION: ALLY-3 PHASE 3 STUDY. Hepatology 2015; 61: 1127-1135.
- Hezode C, de Ledinghen V, Fontaine H, Zoulim F, Lebray P, Bourliere M, et al. Daclatasvir Plus Sofosbuvir with or with HCV GENOTYPE 3 INTERIM ANALYSIS OF A FRENCH MULTICENTER COMPASIONATE USE PROGRAM. J Hepatol 2015; 62: S265.
- Gane EJ, Hyland Rh, An D, Svarovskaia ES, Pand PS, Brainard D, et al. Efficacy of Ledipasvir and Sofosbuvir, for 12 Weeks in Patients WITH HCV GENOTYPE 3 OR 6 INFECTION. Gastroenterology 2015. http://dx.doi.org/10.1053/j.gastro.2015.07.063,.
- Pianko S, Flamm SL, Shiffman ML, Kumar S, Strasser Si, Dore GJ, et al. High Efficacy of Treatment with Sofosbuvir + GS-5816 +/- Ribavirin for 12 Weeks in Treatment Experienced Patients with Genotype 1 OR 3 HCV INFECTION. Hepatology 2014; 60: 297A-298A.
- Kohli A, Kapoor R, Sims Z, Nelson A, Sidharthan S, Lam B, et al. LEDIPASVIR AND SOFOSBUVIR FOR HEPATITIS C GENOTYPE 4: A PROOF-OF-CONCEPT, SINGLE-CENTRE, OPEN-LABEL PHASE 2A COHORT STUDY. Lancet Infect DIS 2015; 15: 1049-1054.
- Hezode C, Asselah T, Reddy Kr, Hassanein T, Berenguer M, Fleischer-Stepniewska, et al. OMBITASVIR PLUS PARITAPREVIR PLUS RITONAVIR WITH OR WITHOUT RIBAVIRIN IN TREATMENT-NAIVE AND TREATMENT-EXPERIENCED PATIENTS WITH GENOTYPE 4 CHRONIC HEPATITIS C VIRUS INFECTION (PEARL-I): A Randomized, Open-Label Trial. Lancet 2015; 385: 2502-2509.
- Younossi ZM, Stepanova M, AFDHAL N, KOWDLEY KV, Zeuzem S, Henry L, et al. Improvement of Health-Related Quality of Life and Work Productivity in Chronic Hepatitis C Patients with Early and Advanced Fibrosis Treated with Ledipasvir and Sofosbuvir. J Hepatol 2015; 63: 337-345.
A retrospective study of chronic hepatitis C (hg c) suggests that on average, 20% of patients have been developing cirrhosis of the liver (CPU) for 20-30 years. The rate of formation of cirrhosis depends on a number of factors. Slow increase in fibrosis with xg C is observed in women of young age in the absence of factors such as liver steatosis, iron overload syndrome, alcohol abuse. A number of reasons determine the rapid formation of the CPU: an elderly age in infection, the male floor, the systematic use of alcohol more than 50 g / day, the presence of coinfection of hepatitis V viruses and / or HIV, excess body weight (\u003e 28 kg / mi), heterogeneity in hemochromatosis gene, The polymorphism of the genes of a series of cytokines playing a key role in fibrgenesis. The average time for the development of the CPU in persons infected at the age of 40 years and abuse of alcohol is 13 years old, and young women in the absence of alcohol intake, the CPU is formed after 42 years. In 32% of patients with XG C flows stably and is not accompanied by the progression of the disease.
An important factor in fibrgenesis is the persistent activity of the XG C on laboratory data and morphological features. In patients with a persistent normal level of serum transamaminases, the risk of developing CPU C is 5%, while the presence of a 3-5-fold increase in the alt of serum is associated with the rapid formation of the CPU with in 50% of patients. It is also shown that the risk factors of the progression of fibrosis are: the presence of fibrosis in the liver tissue at the first biopsy, the heap steatosis and the age of patients. The speed of the progression of fibrosis is determined by the preceding fibrosis, steatosis and lobular hepatitis. With a low degree of activity (yoke on Knodell 4-8 points), the risk of developing CPU with 7-10% of patients, with a high degree of activity (yoke - more than 13 points) in 71% of patients with cirrhosis can develop after 7 years . Prospective study of 404 patients with a compensated CPU with showed that in 85.7 ± 36 months of observation in 28% of patients develop at least one complication of CPU C, including hepatocellular carcinoma (ICC) - in 19%, ascites - 17%, bleeding Of the varicose extended veins of the esophagus (VRRP) - in 5%, the decompensation of the CPU C (Child in / s) is 17%, encephalopathy - in 2%.
The high frequency of the development of the CPU with a chronic HCV infection and the risk of serious complications in this group of patients determines the problems of antiviral therapy (PVT). The main task of treatment is the eradication of the hepatitis C virus and the achievement of the resistant XG C, however, the possibility of achieving a sustainable virological response (WEV) in patients with CPUs with significantly lower than with XG S. Studies of recent years have shown that PVT contributes to a decrease in fibrosis severity, so Patients with CPU with without a virological response The purpose of antiviral treatment is the slowdown in the progression of the disease, a decrease in the risk of decompensation of the CPU and the development of its complications, including the GCC, B-cell lymphoma, cryoglobulinemia, extrahepatic manifestations, portal hypertension and liver and cellular failure.
Presents the interest of the study M. Curry and co-authors (2005), which have studied the effect of long-term therapy by Peginterferon α-2B in small doses on the dynamics of portal hypertension in patients with XG C with the FIBROS stage F3 and CPU C (F4). The Copilot study included 267 patients receiving colchicine 0.6 mg 2 times a day, and 270 patients who are treated with Pengintron 0.5 μg / kg once a week for 4 years. Both groups were represented by patients who did not respond to interferon and ribavirine therapy. 83% of patients in each group had CPU C, 40% of them had signs of portal hypertension identified during endoscopy (VRP or portal gastropathy). EGDs was conducted with an interval of 2 years. Published preliminary results of the study.
In 5 patients with CPUs, which did not receive β-blockers in order to correct portal hypertension, portal pressure was measured before treatment. After 2 years of treatment, with re-EGDs, new VRRPs appeared in 11 of 66 patients who received colchistes, and persisted in 5 of 66 patients who received the monotherapy of Pengintron. In all 5 patients, the initial portal pressure was 15 mm RT. Art., After 24 weeks, the treatment was an average of 6 mm Hg. Art. Bleeding from VRVP after 2 years was noted in 11 (9%) patients receiving colchicine, and at one (1%) of the patient who received the pegintron. Ascites and liver cellular insufficiency were also more often detected in the treatment of colchicine (20 patients) than a pegintron (13 patients). Thus, long-term treatment with small doses of the pegintron of patients with CPU C can slow down the formation of VRPP, reduce portal pressure, prevent bleeding from VRPP and other complications of portal hypertension in patients with CPUs that have not achieved by ISVI on the preceding combined interferon and ribavirine therapy.
In recent years, PVT has undergone significant changes: since 2000, the combined therapy by the pegilated interferons α-2a and 2B and Ribavirin took leading positions in the treatment of XG C and the compensated CPU CPU. The prognostic factors of response to treatment have been studied, the possibilities of correction of a number of side effects of PVT have appeared, What made it possible to achieve WEV in 56-63% of patients with hg with included in treatment. The commitment of patients with treatment, adequate doses of drugs and the duration of PVTs allow you to increase uvo to 72-75%. The greatest effect of combination therapy Xg C is noted in patients with 2 or 3 HCV genotypes: a short treatment course (24 weeks) at high adherence to the treatment of pegylated IFN α and ribavirin allows you to achieve success in 84-94% of cases.
The mandatory purpose of the combined PVT (IFN α and Ribavirin) is promoted to increase the efficiency of PVT, the choice of optimal doses of drugs and the duration of treatment depending on the HCV genotype and the viral load. In addition, the correction of the factors of an unfavorable response to treatment (steatosis, cholestasis, iron overload syndrome) and side effects of PVT (depression, hemolytic anemia when using ribavirin, leo-and thrombocytopenia in the treatment of IFN α, thyroid dysfunction). Suboptimal doses of drugs used in the conduct of PVT, and insufficient duration of treatment contribute to the formation of a group of resistant to antiviral therapy of patients with XG C, which makes it necessary to conduct repeated PVT courses. Thus, it was shown that with a 48-week combined PVT IVI, 72% of patients with 1B HCV genotype and low viral load were achieved. The subsequent aggravation of Hg C was noted in 3% of patients. At the same time, with a 24-week PVT, UVV was observed only in 51% of patients with the specified category, and the aggravation of XG C and the resumption of Virhmia after 6-18 months after the end of the PVT was observed in 40% of patients.
Despite the achievements of recent years, there are categories of difficult to treat patients with xg C, which include patients with 1 HCV genotype and high viral load and patients with CPC CP.
HCV genotype 1 and high viral load turned out to be independent prognostic factors of a weak response to treatment. The reasons for this are not clear. The value of mutations in E2 and NS5A HCV genes is studied (NS5A unstructured region determines the sensitivity to interferon). Elimination of hepatocytes infected with 1 HCV genotype in the process of PVT is slower than with other genotypes. In the first 1-2 week of therapy, the viral load is reduced by 1.6 log copies / ml with genotype 1 HCV and by 2.9 Log copies / ml during genotype 2. The death rate of infected hepatocytes is 0.1 per day in patients with genotype 1 and 0.26 per day with Genotype 2, which is explained by differences in the immune response in patients and gives grounds for discussing the need for more aggressive and, possibly longer PVT in genotype 1 HCV.
The strategy for the treatment of patients with CPU and XG C, infected with 1 HCV genotype and having a high viral load, closely related. UVV in the treatment of IFN α in the standard mode of patients with xg C with Gotype 1 HCV does not exceed 10% regardless of the terms of treatment - 24 or 48 weeks. When using combination therapy (IFN α / ribavirin), for 48 weeks, uvo in such patients, up to 28-36% increase in such patients, remaining significantly lower than WSV with genotypes 2 and 3 HCV (64-79%). Treatment xg C with genotype 1 HCV for 48 weeks high results (46-52%) than 24 weeks (29-42%). Thus, the HCV virus genotype determines the PVT strategy with C and CPU C.
The level of viral load, as well as the virus genotype, does not affect the option and severity of the flow of XG C. High viral load (more than 2x10 6 copies / ml or more than 800,000 me / ml) can be detected in chronic hepatitis low, moderate, high degree of activity , with minimal changes in the liver or with CPU C. However, the level of Virymia clearly affects the frequency of achievement of WEVO: a pegylated IFN α-2B 1.5 μg / kg 1 time per week in combination with ribavirine at a dose of 800 mg / day with high viral load Provides uvo in 42% of cases, and at low - 78%.
In recent years, the method has been developed for assessing the success of therapy on the basis of the study of viral kinetics at an early stage of PVT. Early virological response allows you to predict IVV. High commitment to sick hg c to treatment and assessment of the PVT forecast on the basis of the data of an early virological response to the 4th or 12th week, increased the effectiveness of therapy in the group of all treated patients with hg to 90%. The refusal to the standard treatment schemes of the IFN α (3 million IM 3 times a week) with the transition to the combined PVT also contributes to increasing the number of patients with early virological response.
The study of an early virological response based on a quantitative analysis of HCV-RNA using highly sensitive PCR allows you to identify patients who do not respond to PVT. If, after a 12-week PVT, the hyphenous HCV-RNA levels decreased by two or more decimal, the HCV RNA level, but the RNA of the virus is still detected in the blood, then it is advisable to continue PVT for another 12 weeks, and then re-examine the HCV RNA. With its negative result, IVV varies from 42 to 78%, depending on the viral load. It seems the appropriate 72-week rate of PVT, that is, the extension of treatment is up to 1.5 years, which makes it possible to significantly improve the results of treatment. Under preserving viremia with a drop in its level on the 12th week in less than two decimal logarithm of uvo ranges from 0 to 5%, which is already in early stages or refuse to be unpromising therapy in genotype 1 HCV, or modify it or go to support Therapy of the pegylated IFN α-2a (90 μg) or IFN α-2B (0.5 μg / kg) in order to slow down the progression of the CPU C and the prevention of the development of the ICC and lymphoma.
Thus, genotype 1b and high viral load define the category "difficult" for the treatment of patients with CG C. Regarding this group of patients, it is necessary to strictly follow the rule of the maximum efficient doses of pegylated IFN α-2B (1.5 μg / kg) or IFN α- 2a (180 μg) in combination with ribavirine in a dose above 13 mg / kg with duration of treatment 48-52 weeks. It is known that the pegylated IFN α-2a and 2b differ from each other by pharmacokinetics and pharmacodynamics. An independent comparative assessment of the kinetics of a virological response to the pegylated IFN α-2a in a dose of 180 μg / weeks and IFN α-2B at a dose of 1.5 μg / kg / week was combined with a ribavirine at a dose of 15 mg / kg / day at the primary Patients with CG C. At the end of the course of treatment, the virological response to the combined therapy of the PAGIFN α-2A / ribavirine, and the α-2B / ribavirine peripherals in patients with 1 HCV genotype was 55% and 76%, respectively, which makes it possible to recommend the use of the OGIFN α-2B Combined PVT in this category of patients. Currently, a number of authors propose to evaluate the early virological response to the 4th week and in the absence of a virological response to modify the treatment. The induction therapy of the pegylated IFN α-2B is used at a dose of 3 μg / kg / weeks within 4 weeks or 2 μg / kg / weeks for 8 weeks, followed by the use of the drug at a dose of 1.5-1.0 μg / kg / week.
The triple scheme of the combined PVT with the inclusion in addition to the pegylated IFN α and Ribavirin 200 mg of Amantadin does not have the advantages over the usual scheme in the treatment of XG C genotype 1b with high viral load.
In 2004, preliminary results of the treatment of patients with a hynotype of 1 HCV and high viral load that did not respond to the first rate of PVT IFN α and ribavirin, a combination of α-thymosin-1 (1.6 mg 2 times a week subcutaneously), a pegylated IFN α -2A (180 μg per week) and ribavirin (1000-1200 mg / day) within 24 weeks. An early virological response to the 12th week of treatment is achieved in 47.8% of patients, the virological response after 24 weeks remained in 39.1% of patients with C representing the "difficult" group to treat. An additional preparation (α-thymosin-1) did not add new side effects and was well tolerated by patients.
New strategies in the treatment of "difficult" patients with 1 HCV genotype and a high viral load include the extension of a combined PVT durations to 72 weeks in patients who have not reached an early virological response at the 4th week, which allows you to increase WEV with 22% (at 48-week Therapy) up to 51% and reduce the frequency of exacerbations.
The rationale for the treatment of XG C with an advanced stage of fibrosis or a generated CPU with has become data to reduce the risk of decompensation of the CPU and the development of the CPC, as well as the regress of fibrosis in 60% of patients receiving PVT. The presence of portal fibrosis or CPU C is considered an independent low-frequency factor in HCV-infected patients. Patients with CPU C are usually poorly responded to a standard IFN monotherapy α: uvo ranges from 5 to 20%. The effectiveness of combination therapy of the IFN α and Ribavirin was 5-29% in this group. The use of pegylated IFN α in the composition of combined therapy of a compensated CPU C or xg C with bridge-like fibrosis made it possible to increase uvo to 44-50%.
It should be noted that even with monotherapy of a pegylated IFN α, a histological improvement can be achieved in 54% of patients with a compensated CPU CPU. In a comparative study of the effectiveness of pegylated IFN α-2a and 2b in patients with CPU C, the presence of bridge fibrosis was a negative prognostic factor to achieve an early virological response. At the end of the 24-week PVT, the virological response in the 1st group of patients with CPU C amounted to 83%, in the 2nd - 60%. Thus, the pegylated IFN α-2a may be a drug selection in combination therapy CP CP. Even in the absence of a virological response to a combined PVT at CPU C, there is an improvement in the histological picture in the liver (decrease in yoke and GIS).
The most significant improvement in morphological data takes place when achieving IVV, which is accompanied by improving the quality of life of patients with CPU C, despite the presence of an advanced stage of the disease. The interest of Poynard and co-authors (2000), observing 3010 patients with Xg C with repeated liver biopsy (before the start of PVT and after 6-12 months after its end), when using various treatment modes: IFN monotherapy α-2B, combined PVT IFN α or Pegylated IFN α-2B and ribavirine for 48 weeks. More than a third of the patients who have been achieved by WEV, the histological picture (GIS and IGA) improved in the liver, the morphological speaker is also marked in a third of patients without a virological response. Analysis of liver biopsies in patients with hg with participating in four multicenter studies, showed that 75 (49%) of 153 patients with CPU C after the end of the GIS Therapy (fibrosis level) decreased by 1-3 points, which allows us to talk about the possibility of fibrosis regression With CPU with under the influence of persistent targeted PVT.
In recent years, attempts have been attempts to antiviral treatment of decompensated CPU C (Child in and C). It is known that 40% of all orthotopic liver transplants are carried out in connection with CPU C. Patients with continuing viremia have high risk Transplant reactions and infection of the donor liver with a hepatitis C with rapid development (within 5-7 years) CPU C and / or HCC in a transplanted liver. In 2003-2004 The first publications of the use of PVT with small doses of interferon and ribavirin with a decomposed CPU with the candidates for liver transplantation are appeared. It is proposed to begin treatment of IFN α 3 million me daily and ribavirine 800 mg / day in 4 months before the intended operation. The daily administration mode of interferon allows to reduce the frequency of flu-like syndrome, treatment for 4 months allows to achieve maximum decrease in viremia (before surgery). In 9 (30%) of 30 patients with decompensated CPU C (Child in or C), it was possible to achieve a virological response to the 12th week, 6 of them (20%) avialimius remained after the liver transplantation. Similar data on the possibility of developing UVV in 18-20% of cases of decompensated CPU with a number of authors are published, the duration of observation of such patients continues more than 3.9 years.
It is known that alcohol use significantly increases mortality in viral CPU: five-year survival of patients reaches only 43%, significantly different in CPU groups (66%), Child in (50%) and Child C (25%). With the continuing intake of alcohol, the risk of death in patients with CPU C is increasing in the case of factors such as elderly age, liver cellular dysfunction (Child in or C), gastrointestinal bleeding, coinfection (HBV, HCV), smoking and lack of signs of acute alcoholic hepatitis With liver biopsy. Among the mechanisms of the influence of alcohol on the progression of HCV infection, the activation of replication, increasing the diversity of quasivides and mutations of the virus, enhancing the apoptosis of hepatocytes, suppression of the immune response of the owner, the increase in steatosis and iron levels in the liver is noted. All this leads to a rapid development of the disease, a high frequency of the formation of CPU C and HCC and the low efficiency of interferonotherapy. The effectiveness of PVT with xg C in individuals consisting of alcohol, 3 times lower than standard WSV indicators: with monotherapy, IFN WEV is reduced to 7-8% compared with 25% in patients who do not consume alcohol; With combination therapy - up to 12-4% compared with 41%. There are no safe doses of alcohol for patients with XG C. It is recommended to complete rejection of its reception in 6 months before the alleged PVT, which improves the results of antiviral treatment, but WSV does not reach indicators inherent in patients who did not use alcohol in the past. Return to the reception of alcohol after the end of PVT increases the risk of exacerbation of the XG C and the return of Virhia.
In patients with hg s at the stage of cirrhosis or in the presence of bridge fibrosis (F3), the risk of developing side effects of interferonotherapy is higher than at less advanced fibrosis stages. It is shown, however, that the frequency of their detection and the need to stop PVTs are not significantly different in groups of patients treated with pegylated IFN α or IFN α in standard mode. The pegylated IFN α-2a has a more pronounced myelosuppressive action than the IFN α-2B. Hematological toxicity When using pegylated IFN α is manifested in the first 4 weeks of treatment, then a steady level of leukocytes and platelets is achieved. Especially quickly their number is reduced after the first dose of drugs. PVT is prescribed with a patient with compensated CPU with with a leukocyte level of 3000 / MMH and platelets 50,000 / mm. With a decrease in the level of neutrophils up to 600 / mm, and platelet levels up to 20,000 / MMH, IFN α cancel.
The dose of the pegilated IFN α or ribavirin (reduction of the dose or the abolition of the drug) due to side effects was noted in 50% of patients with CPU C. Depending on the achievement of an early virological response at the 12th week of treatment, various treatment options were proposed with: continued combination therapy in the most effective doses for 36 weeks when the early virological response is reached; Treatment with small doses of pegylated IFN α-2B (0.5 μg / kg) for 5 years in the absence of such an answer in the 4th week (Epic3) or low doses of the pegylated IFN α-2A (90 μg) for 4 years (Halt -FROM).
Defined indications for repeated courses of PVT: the presence of genotypes 2 or 3 nsv; Partial response at the previous PVT, F3 and F4 stage of fibrosis. Contraindications to repeated treatment courses are: elderly age, genotype 1, CPU with hyperbilirubinemia, high viral load, high body weight index, minimal changes in the liver during biopsy (yoke less than 4 points) and continued alcohol or drug use.
Thus, PVT compensated and decompensated CPU at xg with solves a number of the following tasks: a slowdown in the decompensation of cirrhosis, a decrease in mortality from its complications (bleeding from varicose extended veins, hepatic cell failure, etc.), preventing the development of the ICC and the prevention of reactivation of infection After liver transplantation, as well as improved quality of life of patients and ensuring their social rehabilitation. There is no doubt that in the early stages of HCV infections of PVT gives the best results: the frequency of UVV in the treatment of acute hepatitis C reaches 90%, Xg C - 60-70%, which exceeds the effectiveness of the treatment of CPU with pogilaned IFN α and ribavirin (30-50%) . Our experience of PVT hg with a low degree of activity allows us to talk about the high effectiveness of the treatment of this category of patients. Using the pegylated IFN α-2B (1.5 μg / kg) and ribavmerin (more than 10.6 mg / kg) in the treatment of primary patients with a small period of the disease (5.9 ± 5.7 years), mostly low degree of activity and weak Fibrosis (F1), as well as low viral load, we obtained a steady virological response in 86% of cases, including 77% of patients with 1 HCV genotype, including 5 patients at the CPU stage.
Literature
- Collier J. D., Woodall T., WIGHT D. G. D. et al. Predictiv of Progressive Hepatic Fibrosis Stage On Sabsequent Liver Biopsy in Chronic Hepatitis C Virus Infection. J. Viral Hepatitis, 2005; 12: 74-80.
- Niederau C., Lange S., Heintgest T. et al. Prognosis of Chronic Hepatitis C: Results of a Large, Prospective Cohort Study. Hepatology, 1998; 28: 1687-1695.
- Curry M., Cardenas A., AFDHAL N. H. Effect of Maintenance PEG-Intron Therapy On Portal Hypertension and Its Complications: Results from The Copilot Study. J. Hepatol., 2005; 42 (2): 95.
- Fried M. W., Shiffman M., REDDY R. et al. Peginterferon Alfa-2a Plus Ribavirin for Chronic Hepatitis C Virus Infection. N ENGL J. MED., 2002; 347: 975-982.
- Manns M., Mchutchison J., Gordon S. et al. Peginterferon Alfa-2B Plus Ribavirin Compared with Interferon Alfa-2B Plus Ribavirin for Initial Treatment of Chronic Hepatitis C: A Randomized Trial. LanCet, 2001; 358: 958-965.
- Luise S., Bernardinello E., Cavalletto L. et al. Kinetic of Virolological Response Duning Peg-IFNS in Chronic Hepatitis C. J. Hepatol 2004; 40 (1): A 490.
- BERG T., VON WAGNER M., HINRICHSEN H. et al. COMPARISON OF 48 OR 72 WEEKS OF TREATMENT WITH PEATIRFERON ALFA-2A (40 KD) (PEGASYS) Plus Ribavirin (Copegus) in Treatment-Naive Patients with Chronic Hepatitis C infected with HCV GENOTYPE 1. HEPATOLOGY 2003; 38 (1): 317A.
- Hadziyannis S. J., Papatheodoridis G. V. PEGINTERFERON- (2A (40 KDA) for Chronic Hepatitis C. Expert Opin. Pharmacother. 2003; 4: 541-551.
- Poynard T., Marcellin P., Lee S. S. et al. Randomised Tial of Interferon Alpha 2B Plus Ribavirin for 48 Weeks OR for 24 Weeks Versus Interferon Alpha 2B Plus Placebo for 48 Weeks for Treatment of Chronic Infection with Hepatitis C Virus. LanCet 1998; 352: 1426-1432.
- Poynard T., Mchutchison J., Manns M. et al. Impact of Pegylated Interferon Alpha-2B and Ribavirin On Liver Fiber Hepatitis C. GastroNerol. 2002; 122: 1303-1313.
- Forns X., Navasa M., Rodes J. Treatment of HCV INFECTION IN PATIENTS WITH ADVANCED CIRRHOSIS. Hepatology, 2004; 40: 498.
- Nikulkina E. N., Kret P. E., Lopatkin T. N. et al. Combined therapy by Peginterferon Alpha-2B (Pengintron) and Ribavirin (Rebiquol) in primary patients with chronic hepatitis C // Clinical pharmacology and therapy. - 2004. - № 13 (2). - P. 48-52.
T. N. Lopatkin, candidate of Medical Sciences, Associate Professor
MMA them. I. M. Sechenova, Moscow
Citation:Nadinskaya M.Yu. Treatment of chronic viral hepatitis // RMW. 1999. №6. P. 4.
Treatment of viral hepatitis, taking into account the level of morbidity, the frequency of disability and mortality has important medical and socio-economic importance. Today, hepatitis V viruses in, C and D are the most frequent cause chronic hepatitis, liver cirrhosis and hepatocellular carcinoma (HCC). The purpose of the therapy of chronic viral hepatitis is the eradication of the virus, slowing the progression of the disease and reduce the risk of the development of the ICC. The only drug with proven effectiveness in the treatment of chronic viral hepatitis is interferon-a. When applied, a persistent answer is achieved in 25-40% of patients with chronic hepatitis B, 9-5% chronic hepatitis D and 10-5% chronic hepatitis C. New direction in the treatment of chronic viral hepatitis is the use of nucleoside analogues: lamivudine and phambyclovir in the treatment Chronic hepatitis B and ribavirin in combination with interferon in the treatment of chronic hepatitis C.
Interferon. Interferons (IFN) are glycoprotein cytokines that have antiviral, immunomodulatory and antiproliferative activity. These cytokines are produced by immune cells in response to virus antigens. Interferons inhibit viruses replication, increase the expression of HLA I class antigens (main complex histocompatibility) on the cell surface, stimulate the ripening of cytotoxic T cells and enhance the activity of NK cells (natural killers). These mechanisms provide the purification of infected cells from the virus. In addition, recently data appear indicating that the IFN slows down fibrgenesis in the liver. This is due to a decrease in the activity of the inflammatory process in the liver as a result of the eradication of a viral infection, so with the direct influence of IFN on the synthesis of collagen.
There are two types of IFNs. To i type include IFNa and IFN-B to the second - IFNg. The greatest effectiveness in the treatment of chronic viral hepatitis showed IFN-A . Applied both leukocyte (natural) and recombinant drugs of the IFNa. The latter got the greatest distribution. Info-a preparations are applied parenterally - subcutaneously or intramuscularly, and the advantages of any of these two methods of administration are not established.
The answer to the therapy of IFN
The main indicators of the effectiveness of the IFN-A therapy are: the disappearance of the virus replication markers and the normalization of the level of the alanine transaminase (ALT). Depending on these indicators by the end of treatment and after 6 months after its completion, several types of response are distinguished:
1. Resistant answer. It is characterized by the disappearance of the markers of the replication of the virus and the normalization of the level of Alt during treatment and within 6 months after the end of the course of therapy.
2. Unstable (transit) answer. During treatment, replication markers disappear and the level of ALT normalizes, but for 6 months after the cessation of treatment develops a relapse.
3. Partial answer. Against the background of treatment, there is a decrease or normalization of the indicators of Alt, and markers are saved replication.
4. No response. The virus replication and the elevated level of Alt are preserved.
The value of the resistant response reflects the effectiveness of interferonotherapy. If the relapse did not occur after 6 months after the completion of the course of treatment, the likelihood that it will happen in the future, is small.
In cases where the persistent answer is not reached and recurrence is developing, a re-treatment is carried out.
In case of incomplete answer or its absence, the dose correction is carried out or the combined treatment regimens are applied.
Contraindications for the treatment of IFN
a.
Chronic viral hepatitis:
1. Decompensated liver cirrhosis.
2. Heavy somatic diseases.
3. Thrombocytopenia< 100 000/мл.
4. Leukopenia< 3000/мл.
5. Continuation of drug use or alcohol.
6. The presence of a history of mental illness (especially severe depression).
Given the high risk of developing the ICC, patients with liver cirrhosis should be considered as candidates for IFN-A therapy. Interferonotherapy with this patient is carried out if the synthetic function of the liver is preserved, the platelet count of more than 100,000 / ml, leukocytes more than 3000 / ml, there are no indications of the complications of the cirrhosis (bleeding from varicose veins of the esophagus, ascites, hepatic encephalopathy) and there is no significant increase in level A -Phetoprotein.
Side effects in the treatment of IFNa.
The most frequent side manifestation in the treatment of IFN-A There is a so-called flu-like syndrome, which develops after 3 - 5 hours after the administration of the drug and is characterized by increasing the temperature, Malgia, arthralgia, headache. This syndrome is most difficult after the first injection and is usually significantly reduced during the 1st and 2nd weeks of treatment. The severity of the syndrome can be significantly reduced by the use of IFN before bedtime and the purpose of paracetamol and / or non-steroidal anti-inflammatory drugs during the introduction of the IFN and the next morning.
The frequent side complications include a decrease in platelets and leukocytes, which The most pronounced in patients with cirrhosis of the liver and is usually developing on the 2nd - 4th month of treatment. With the appearance of pronounced thrombocytopenia and / or leukopenia, reduce the dose of IFN.
Rare side manifestations are a decrease in appetite and loss of body weight during treatment that do not require cancellation. The depression is also related to the number of rare adverse reactions, which more often develops in patients having a burdened mental history. With the development of depression, treatment must be discontinued. Therefore, patients with depression in history should be inspected by a psychiatrist before the start of treatment.
Autoimmune complications when applying infra Rarely develop, but their occurrence requires cancellation.
Treatment of chronic hepatitis C
The hepatitis C virus is the leading cause of chronic hepatitis and the ICC, as well as leading to the development of decompensated cirrhosis, the most frequent indication to the conduct of liver transplantation. According to WHO, about 1% of the population of the world is infected with the hepatitis C virus in the Russian Federation, the incidence of hepatitis C is registered since 1994, while its significant increase (for the period from 1994 to 1997, the incidence increase was 180%). The greatest morbidity is celebrated in adolescents and young people.
In the works that investigated the natural evolution of hepatitis C viral infection is shown that the time passing from the beginning of infection to the development of clinically significant hepatitis is an average of 10-20 years, to the development of the liver cirrhosis - more than 20 years and to the development of the ICC - about 30 years. These data, as well as an increase in infection with the hepatitis C virus and the lack of effective immunoprophylaxis involve the continuation of the growth of morbidity and mortality from liver cirrhosis due to this virus, in the next 10-20 years.
The purpose of treatment Patients with chronic hepatitis C is the eradication of the virus, slowing the progression of the disease and reduce the risk of developing the ICC.
Indications for conducting therapy infraa.
Patients with chronic hepatitis C: the detection of HCV RNA in the blood and an elevated level of Alt.
Factors predicting a good answer to the therapy of infractions
a.
:
short period of the disease, young age, lack of cirrhosis, low HCV RNA level (< 10 5 k / ml), HCV 2 - 6 genotype, HIV negativeness, female floor.
The most important response factor is the virus genotype. The smallest treatment efficacy is achieved in patients infected with genotype 1b. This genotype in the Russian Federation accounts for about 70% of all cases of infection. With prolonged treatment, part of patients with genotype 1b can achieve a resistant response.
The next most common treatment scheme: 3 II 3 times a week for 6 months. Monitoring of patients, including clinical analysis (the number of leukocytes and platelets) and biochemical research (transminase) are carried out on the 1st, 2nd and 4th weeks of treatment, then every 4 weeks before the end of the course of therapy.
When applying the described treatment regimen, the Eradication of HCV RNA and the normalization of Alt to the completion of the treatment course is achieved in 30 - 40% of patients, but most of them have a recurrence over the next 6 months and a resistant response value is 10 - 20%. An increase in the resistant response can be achieved by an increase in the duration of interferonotherapy from 6 to 12 months or an increase in doses of IFNa. In the first 3 months of treatment up to 6 and 3 times a week.
The first assessment of the effectiveness of treatment is carried out after 3 months from the beginning of the treatment of IFNa. . This is due to the fact that 70% of patients who manage to achieve a resistant response, HCV RNA disappears from the blood during the first 3 months of therapy. Although some HCV PNN patients may disappear in the subsequent period (between the 4th and 6th months of treatment), the likelihood of achieving a resistant response is small.
The latest published studies show that interferonotherapy can slow the development of the liver cirrhosis, to prevent or move the development of the ICC in patients with chronic hepatitis. Therefore, with a high degree of hepatitis activity, when the purpose of interferonotherapy is the slowdown in the progression of the disease, it is necessary to continue therapy of the IFNa.
There are controversial data on the need to treat patients with a normal or slightly increased level of Alt. According to modern ideas, treatment in these patients should be carried out when a high concentration of HCV RNA is found in the blood or the presence of high inflammatory activity in the liver.
Patients who have developed a relapse are repeated course of therapy with the same IFN-A in higher doses (6 IF 3 times a week) or recombinant IFN-A are replaced by leukocytarial. Treatment is carried out for 12 months. The persistent answer is achieved in 30 - 40% of patients.
An alternative scheme in patients with recurrent or not responding to treatment is the use of IFN-A In combination with ribavirin.
Ribavirin is an analogue of purine nucleosis and has a wide range of antiviral activity against RNA and DNA-containing viruses. The mechanism of its action is finally studied. Its damaging effect on viral RNA and synthesis of viral proteins is assumed.
When Ribavirin is used in the form of monotherapy, the concentration of HCV RNa does not occur, although the level of Alt is significantly reduced. With a combined application with IFNa. The magnitude of the persistent answer increases to 49% compared with the use of one IFN. This is due to reducing the frequency of relapses. Doses of ribavirin range from 600 to 1200 mg per day.
The most frequent side manifestation of ribavirin treatment is hemolytic anemia. The average reduction of hemoglobin is 3 g / dl, Although there are cases of decline and more than 5 - 6 g / dl. The reduction of hemoglobin to the level of 8.5 g / dl requires the cancellation of treatment. Other frequent side complications are rash and nausea. It should be borne in mind that Ribavirin is a teratogenic drug, Therefore, women of reproductive age, receiving treatment with ribavirin, should use contraceptives. The duration of teratogenic risk after the termination of therapy with ribavirin is definitely not defined.
In the treatment of chronic hepatitis C are also used other drugs in the form of monotherapy or in combination with IFN-A . These include: antiviral drugs - amantidine; cytokines - granulocyte-macrophagative stimulating factor and thymbosin A1; Ursodeoxycholic acid. In order to reduce iron content, phlebotomy is used. But none of these agents showed a significant effect on the HCV RNA titer in the blood or to slow down the progression of the disease.
Approaches to the treatment of chronic hepatitis C with the coinfection of the hepatitis G virus do not have significant differences from those for chronic hepatitis C without coinfection.
Further directions along the way to increase the effectiveness of the treatment of chronic hepatitis C include the study of HCV inhibitors of proteases - Helikaz, as well as the study of the modification of the IFNa with a long chain polyethylene glycol attached to it. This modification increases the half-life of interferon from 6 hours to 5 days, which allows you to assign this drug once a week. Currently clinical studies are held.
Decompensated liver cirrhosis in patients with chronic hepatitis C is an indication for liver transplantation. In most countries from 20 to 30% of all liver transplants are carried out on this issue. After transplantation, most patients develop a recurrence of HCV infection in the donor liver. However, this does not affect the frequency of transplant rejection and survival in comparison with transplants conducted for other reasons. In the post-transplantation period for the treatment of viral hepatitis with IFN-A One or in combination with ribavirin has a limited meaning.
Specific prophylaxis of chronic hepatitis C currently does not exist. Large genetic heterogeneity of the virus genome and the high frequency of mutations make significant difficulties in creating a vaccine.
Treatment of chronic hepatitis in
The frequency of the infection of the HBSAG population is subject to significant fluctuations depending on the geographical area and averages 1-2%. In the Russian Federation in recent years, there has been a tendency to increase the incidence of hepatitis B.
The goal of therapy Chronic hepatitis B is the achievement of seroconversion and elimination of HBSAG, slowing down the progression of the disease and reducing the risk of developing the ICC.
Indications for interferonotherapy: Detection of HBV replication markers - HBEAG, HBCAB IGM, HBVDNA and elevated alt.
: The level of Alt, which exceeds the norm 2 times or more (compared to the normal level of Alt, the value is increased by 2 times), short history of the disease, the low level of HBv DNA (level less than 200 PG / ML increases the response 4 times), the absence of Anamnesis of instructions for intake of immunosuppressors, the presence of histological signs of activity, HIV negativeness.
The first assessment of the effectiveness of treatment is estimated at the occurrence of seroconversion - the elimination of HBEAG and the appearance of anti-low. Almost simultaneously with HBEAG, the disappearance of the HBV DNA occurs. During the occurrence of seroconversion (2nd - 3rd month of treatment), there is an increase in the level of transaminase in 2 - 4 times relative to the original, which reflects the immunologically conditioned elimination of HBV. The strengthening of the cytolytic syndrome is usually asymptomatic, however, individual patients comes clinical worsening with the development of jaundice and in some cases of hepatic encephalopathy.
Most often used next the diagram of treatment of IFNa.
: 5 meters daily or 10 hours 3 times a week. Duration of therapy 16 - 24 weeks. Patient monitoring is carried out weekly during the first 4 weeks of treatment, then every 2 weeks for 8 weeks and then 1 time in 4 weeks. The clinical state is controlled, the number of blood formation elements and the transaminase level.
When applying the above treatment schemes, the transient response is achieved in 30 - 56% of patients. The resistant answer is noted in 30 - 40% of patients. The disappearance of HBSAG is achieved in 7 - 11%. The most resistant response is reduced by infection with the mutant strain HBV (when HBeAg is not detected), as well as in patients with cirrhosis of the liver and at low source biochemical activity.
Treatment of patients with cirrhosis of the liver, due to HBV, is carried out by lower doses of IFN-A (3 IM 3 times a week), for a long time - 6 - 18 months.
Regarding the use of prednisolone to increase the effectiveness of treatment in patients with initially low levels of Alt there is no unambiguous opinion. Using a preliminary treatment rate of prednisone (scheme: 2 weeks in a daily dose of 0.6 mg / kg, 1 week at a dose of 0.45 mg / kg, 1 week at a dose of 0.25 mg / kg, then cancellation and after 2 weeks are assigned IFN-A. ) showed an increase in the effectiveness of treatment. However, 10 - 15% of patients with its use leads to the development of decompensation of the disease and the impossibility of further interferonotherapy.
If seroconversion does not occur during the first 4 months of treatment or in patients with a complete initial response develops a relapse, then there is a need to adjust the treatment regimen or re-courses of therapy. For this purpose, Lamivudine or Foscicovir is used. These drugs are used both separately and in combination with IFN-a.
Lamivudine and Famciclovir are antiviral activity preparations and are the second generation of nucleoside analogues. They only act on DNA-containing viruses. Their advantage over IFN-A is the ease of use (drugs are used inside) and the presence of a significantly smaller amount side effects (weakness, headache, Malgia, abdominal pain, nausea, diarrhea).
There are limited data on the use of these drugs in the treatment of chronic hepatitis V. In the first year of treatment with lamivudine, its effectiveness is similar to that IFN-A. When conducting repeated courses of treatment, the use of lamivudine in combination with IFN-A It leads to seroconversions only in 20% of patients.
In the treatment of chronic hepatitis, other drugs are also used, such as levamizol, thymbosin-a 1, cytokine complex. From this group of drugs, thymosin-a 1 - polypeptide of thymic origin is most widely used. It has 35% homology with the C-terminal region of IFN-A which is considered as an important component responsible for the antiviral effect. In preliminary studies, recombinant thyminesina 1 showed the effectiveness similar to such IFN-A Associated response.
In patients with decompensated HVV cirrhosis effective way Treatment is liver transplantation. At the same time, it is necessary to take into account the high risk of developing viral hepatitis B in donor liver in post-transplantation period.
Specific prophylaxis of chronic hepatitis B includes the use of a vaccine.
Treatment of chronic hepatitis D
The frequency of detection of the hepatitis D virus in patients with positive HBSAG is approximately 5 to 10%. The possibility of the development of hepatitis D should be assumed in all patients with chronic HBV infection.
The goal of therapy - Elimination of HDV RNA and HBSAG, reduction of disease progression.
Indications for therapy of the IFNa. : The presence of anti-HDV and HDV RNA in patients with compensated liver disease and signs of biochemical activity. Along with HDV RNA, confirming the test HSD is the detection of HDAG in the liver tissues.
Persistent response factors, not installed. Preliminary studies have shown that HIV-infected with the treatment of chronic hepatitis D corresponds to those in patients without HIV infection.
The following IFN-A treatment regimens are usually used. : 5 me daily or 9 months 3 times a week. The duration of therapy is 6 - 12 months. Also use other schemes for the treatment of IFNa. : The first 6 months 10 and 3 times a week, then 6 months 6 and 3 times a week. Surveillance of patients is carried out according to the scheme of chronic hepatitis V.
The transient response is achieved in 40 - 50% of patients. It is characterized by the disappearance of HDV RNA and the normalization of Alt to the completion of the course of therapy. With further observation, 25% is developing relapse. The resistant answer is noted in 9 - 25% of patients. However, only a small part of these patients (up to 10%) disappears HBsag.
Studies on the use of nucleoside analogues in the treatment of chronic hepatitis D are not completed.
Prevention and role of liver transplantation in the treatment of chronic hepatitis D the same as in chronic hepatitis V.
Literature:
1. Poynard T, Bedossa P, Opolon P, et al. Natural History of Liver FIBROSIS PROGRESSION IN PATIENTS WITH CHRONIC HEPATITIS C. THE OBSVIRC, METAVIR, CLINIVIR AND DOSVIRC GROUPS // LANCET 1997; 349 (9055): 825-32.
2. DATA DATA OF THE FEDERAL CENTER OF GOSANEPIDEDZORE MH RF, 1998.
3. Lviv D.K., Samokhvalov E.I., Mishiro S. et al. The patterns of the spread of the hepatitis C virus and its genotypes in Russia and the CIS countries // Questions of Virology 1997; 4: 157-61.
4. Ouzan d, Babany G, Valla D. COMPARISON OF INITIAL AND FIXED-DOSE REGIMENS OF INTERFERON-ALPHA2A IN CHRONIC HEPATITIS C: A RANDOMIZED CONTROLLED TRIAL. FRENCH MULTICENTER INTERFERON STUDY GROUP // J VIRAL HEPAT. 1998; 5 (1): 53-9.
5. Shiffman ML. Management of Hepatitis C // Clinical Perspectives in Gastroenterology 1998; 6-19.
6. Reichard O, Schvarcz R, Weiland O. Therapy of Hepatitis C: Alpha Interferon and Ribavirin // Hepatology 1997; 26 (3) Suppl 1: 108-11.
7. Malaguarnera M, Restuccia S, Motta M et al. Interferon, Cortisone, and Antivirals In The Treatment of Chronic Viral Hepatitis: A Review of 30 Years of therapy // Pharmacotherapy 1997; 17 (5): 998-1005.
8. KROGSGAARD \u200b\u200bK, MARCELLIN P, TREPO C, ET AL. Pretreatment with Prednnisolone Enhances The Effect of Human Lymphoblastoid Interferon in Chronic Hepatitis B // Ugeskr Laeger 1998 (SEP 21); 160 (39): 5657-61.
9. Mutimer D, Naoumov N, Honkoop P, et al. Combination Alpha-Interferon and Lamivudine Therapy for Alpha-Interferon-Resistant Cronic Hepatitis B INFECTION: Results of a Pilot Study // J Hepatol 1998; 28 (6): 923-9.
10. PUOTI M, ROSSI S, FOREO MA. et al. Treatment of Chronic Hepatitis d with interferon alpha-2b in patients with Human ImmunodeFiciency Virus Infection // J Hepatol 1998; 29 (1): 45-52.
11. Farci P, Mandas H, Coiana A, et al. Treatment of Chrohic Hepatitis D with interferon-2 A // N ENGL J MED 1994; 330: 88-94.