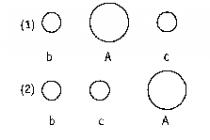
Erectile dysfunction, or impotence (from Latin impotens - powerless) is an integral part of the problem of sexual dysfunctions, the persisting inability to achieve and maintain an erection at the level necessary to ensure a full sexual intercourse.
Erection (from Latin erectio - to straighten) is a neurovascular process that is directly related to the size blood pressure inside the cavernous (cavernous) bodies of the penis. During sexual stimulation, biologically active substances (mainly nitric oxide) are released from the nerve endings, which relax the smooth muscles of the cavernous bodies of the penis, as well as the muscles of the arteries. This leads to vasodilation, increased blood flow in the penis, dilation and filling of the cavernous spaces with blood. At the same time, the veins that perforate the tunica albuginea of the cavernous bodies of the penis are narrowed, and passive venous outflow is hampered.
The most effective exercise to strengthen an erection, squats are considered, it is recommended to perform 50-100 squats a day.
Filling of the cavernous bodies of the penis with blood and veno-occlusion lead to an erection. During intercourse, this state of the vessels remains, the inflow and outflow of blood stops, intracavernous pressure rises. There is an increase in the volume of the penis and a further increase in erection.
Erectile problems over a prolonged period (3–6 months) are grounds for suggesting erectile dysfunction.
According to the WHO, about 160 million men worldwide suffer from erectile dysfunction. Every tenth man over the age of 21 suffers from an erectile dysfunction, about 50% of men over 40 experience various difficulties associated with erectile dysfunction, every third man over 60 is not able to perform sexual intercourse.
Forms
According to the etiological factor, the following types of erectile dysfunction are distinguished:
- psychogenic;
- organic;
- mixed.
Among psychogenic erectile dysfunctions, primary and secondary forms are also distinguished:
- the primary (congenital) form is rare and is characterized by the complete absence of normal sexual function throughout life;
- secondary erectile dysfunction is characterized by the gradual extinction of the previously existing ability to erect.
Erectile Dysfunction Causes and Risk Factors
The causes of erectile dysfunction are subdivided according to the pathophysiological mechanisms underlying its occurrence.
When treating the organic form, it is of paramount importance to eliminate the disease that led to erectile dysfunction.
Organic causes are related to disruptions in performance internal organs or systems. These include:
- vascular. Insufficient blood pressure in the vessels of the arterial bed leads to inadequate blood supply to the cavernous bodies, and the contraction of smooth muscles opens the way for passive venous outflow. Weakening or absence of erections can be a manifestation of arterial hypertension, obliterating endarteritis, hyperlipidemia, atherosclerosis, arterial damage caused by irradiation of the pelvic region, as well as heart failure, coronary heart disease and myocardial infarction;
- neurological. Diseases of the parasympathetic pelvic visceral nerves and pathology of the nerve pathways can lead to impaired redistribution of blood flow, insufficient pressure in the corpus cavernosum, impaired ability to erections. Potency is affected by neurological disorders in Alzheimer's disease, Parkinson's disease, polyneuropathy, multiple sclerosis, hemorrhagic or ischemic stroke, injuries of the spinal cord, small pelvis and perineum, degeneration of intervertebral discs, cerebral insufficiency, etc.;
- endocrine. The causes of impotence of endocrine genesis include increased levels of prolactin, endogenous estrogens and a decrease in the level of androgens, diseases associated with dysfunction of the pituitary and adrenal glands;
- iatrogenic. Explained side effect a number of drugs (antipsychotics, tranquilizers, antihypertensive drugs, anticonvulsants, cytostatics, antidepressants, antihistamines of the 1st generation, corticosteroids, etc.) for sexual function;
- toxic. Due to the toxic effects of alcohol, drugs, nicotine.
The consequence of erectile dysfunction is an unsatisfactory sex life, which leads to further disorders.
Psychogenic causes are associated with central suppression of the erection mechanism. These include increased anxiety, lack of sexual arousal, neuroses, mental illness (depression, schizophrenia). It has been proven that the psychological causes of erectile dysfunction are based on organic diseases. In most patients with erectile dysfunction, a combination of psychogenic and organic components is found.
Aging is an independent risk factor for erectile dysfunction. The leading causes of erectile dysfunction with aging are age-dependent decrease in testosterone levels, vascular pathologies and chronic infectious diseases the urogenital sphere. Sexual disorders progressively increase with aging: in the 50-60 age group, the number of patients is 10%, and after 80 years - already 80%.
Symptoms
Symptoms of erectile dysfunction include:
- insufficient quality morning erections or their absence;
- inability to enter the penis due to insufficient tension;
- premature ejaculation;
- an increase in the time interval between sexual stimulation and erection;
- defective erections or complete absence of an erection upon stimulation;
- inability to introject and maintain an erection until ejaculation;
- decrease in ejaculate volume;
- an increase in the recovery period between erections.
Psychogenic and organic erectile dysfunctions have their own characteristics.
Psychogenic erectile dysfunction begins suddenly. Characterized by the presence of problems in relationships, the presence of nocturnal spontaneous erections. As a rule, erection problems are episodic. After eliminating the external problem, a normal erection is usually restored.
Massage and self-massage of the pelvic and pubic bone area is effective, since it has a beneficial effect on the vascular tone in the genital area.
Erectile dysfunction of organic origin is accompanied by systematic erectile dysfunction. This form of the disease begins gradually and is rarely accompanied by spontaneous nocturnal erections.
Diagnosis of erectile dysfunction
Diagnosis of erectile dysfunction begins with the collection of a general history that identifies etiological factors and an assessment of sexual activity. A number of questionnaires have been developed to identify the pathophysiological basis of impotence.
Physical examination often reveals signs of vascular, neurological or hormonal disorders, confirming the pathophysiological hypothesis based on the history data: the presence of signs of hypogonadism, fibrotic changes, gynecomastia, phimosis, detection of La Peyronie's plaques, disorders of perineal sensitivity, decreased tone of the anal sphincter of the lower extremities, atrophy , changes in peripheral pulsations.
Diagnostics should include screening of major vascular, metabolic and endocrine diseases, determination of testosterone levels.
 Source: umedp.ru
Source: umedp.ru
For an objective assessment of the state of physiological mechanisms that control the process of erection, a number of techniques are used:
- condition assessment vascular system - determination of the level of blood flow in the pelvic arteries using vascular Doppler ultrasonography of the arteries of the penis, plethysmography and radioisotope studies;
- assessment of neurological status- determination of the threshold of sensitivity of the penis to vibration using a biothesiometer (helps to detect early manifestations of peripheral sensory neuropathy), electromyography of the muscles of the perineum, study of the refractoriness of the sacral nerves, registration of brain potentials during irritation of the external genital organs (helps to determine erectile dysfunction of neurogenic origin). If, during screening tests, a neurological pathology is detected in a patient, electroencephalography is performed, CT scan brain or myelography;
- grade endocrine system - measuring the concentration in the blood plasma of the level of testosterone, prolactin, luteinizing hormone;
- grade mental state sick- identification of a psychological, causal relationship (situational impotence), mental disorders (anxiety, depression, feelings of shame, guilt).
Erectile problems over a prolonged period (3–6 months) are grounds for suggesting erectile dysfunction.
For the differential diagnosis of forms of erectile dysfunction, a procedure for evaluating nocturnal erections (NEE) using a plethysmographic sensor is used. The differentiation is based on the fact that patients with psychogenic erectile dysfunction develop normal erections during sleep, while patients with organic erectile dysfunction have inferior nocturnal erections.
Erectile Dysfunction Treatment
The goal of treatment is to achieve satisfactory erections with minimal side effects.
In the treatment of the psychogenic form of erectile dysfunction, psychotherapy plays an important role. It should be aimed at eliminating the causes that led to sexual maladjustment, resolving intrapersonal and interpersonal problems, and forming adequate ideas about intimate relationships. The techniques of matrimonial therapy, training partners in effective interaction, methods of cognitive-behavioral therapy are used.
When treating the organic form, it is of paramount importance to eliminate the disease that led to erectile dysfunction. If impotence has endocrine causes, hormone replacement therapy is prescribed.
Pharmacological agents are widely used to enhance and prolong erection. The first-line drugs are oral PDE-5 inhibitors. PDE 5 is an enzyme found in the cavernous tissue. Blocking its work leads to relaxation of the smooth muscles of the corpora cavernosa and the emergence of an erection in response to sexual stimulation.
It has been proven that the psychological causes of erectile dysfunction are based on organic diseases.
Injection is also possible medicines directly into the corpus cavernosum. In this case, a very thin needle is used, with the help of which the patient can independently inject the vasodilator selected by the doctor. A unilateral injection is sufficient for bilateral enlargement of the penis due to cross blood flow. After 15 minutes, an erection occurs, which lasts up to two hours. The method has disadvantages - inconvenience of use and rare side effects such as priapism and fibrosis of the penis (2%).
Another method of increasing blood flow to the penis is vacuum constrictor therapy. In this case, the use of a vacuum device enhances the blood flow into the cavernous bodies of the penis, and the constrictive ring prevents venous outflow.

In medicine, ischemic stroke means a disorder of cerebral circulation, which is accompanied by signs of neurological pathology. Statistics confirm that stroke is a common reason for recognition of disability in the working-age population over the age of 40.
Functional brain damage has a high mortality rate. Approximately 30% of patients die within a month after suffering an ischemic stroke. Within a year after an acute cerebrovascular accident, more than 50% of patients will die.
The disease negatively affects the state of potency, since a stroke entails life-threatening brain damage and nervous system... Knowledge of the causes of cerebrovascular accident and application preventive measures will allow patients to avoid loss sexual attraction and other serious complications.
Causes of cerebral circulation disorders
Among the negative factors that increase the risk of ischemic stroke, doctors call:
- atherosclerosis of the brain, when the arterial walls are abundantly covered with cholesterol deposits. In patients, there is a significant narrowing of the vascular lumen, a lack of blood supply to the brain. The risk of damage to atherosclerotic plaque increases, this process entails the release of cholesterol and thrombosis of the cerebral arteries;
- atrial fibrillation. An abnormal heart rhythm causes blood clots to move and blockages in an artery in the brain;
- thrombosis of the veins of the lower extremities. Individual blood clots can fragment and clog the vascular lumen;
- thickening of the blood. A high clotting rate increases the likelihood of thrombus formation;
- sharp drops in blood pressure.
The risk group includes middle-aged patients suffering from excess weight, nicotine and alcohol addiction.
Ischemic stroke symptoms
The signs of a vascular disorder differ depending on the form of the stroke. Typically, patients suffer from:
- systemic dizziness when balance is lost while standing, sitting and lying
- lack of coordination of movements and unsteadiness of gait
- paralysis, tremors and loss of sensation
- eye movement disorders
- speech and motor lesions
- disorders of higher nervous activity, in particular, loss of the ability to write, read
Impact of stroke on sexual health
Severe ischemic stroke can cause spinal (cortico-spinal) impotence. Sexual dysfunction involves cases of sexual impotence caused by diseases of the brain and spinal genital centers. The disorder is characterized by exhaustion, decrease or complete loss of excitability.
Depending on the nature of the sexual disorder, spinal impotence can take the following forms:
- increased excitability of the centers affecting erection and ejaculation
- an increase in ejaculatory activity and a decrease in the excitability of the erection center
- lack of excitability of the ejaculatory center - spinal aspermatism
- decreased activity of both centers
Other complications after a stroke
If an ischemic stroke is not fatal, then the patient suffers from:
- cognitive impairment (memory impairment, decreased concentration)
- complete or partial paralysis
- dysarthria, that is, speech disorders (slurred speech)
Prevention of ischemic stroke
To prevent the onset of acute circulatory disorders in the brain and maintain sexual health for a long time, patients are advised to:
- regularly undergo a general medical examination. If among the relatives of the patient, if there are persons affected by a stroke, he should undergo a detailed examination by a cardiologist;
- monitor blood pressure indicators, if necessary, take antihypertensive drugs prescribed by a doctor;
- follow the rules of a balanced diet, limit the use of fried and fatty foods;
- seek medical help in a timely manner when diagnosing cardiac arrhythmias, take antiarrhythmic drugs recommended by a cardiologist;
- control the level of blood clotting with anticoagulants;
- take beds that accelerate lipid metabolism and reduce the activity of the atherosclerotic process;
- if indicated, pass surgery to increase the patency of the arteries supplying the brain.
Erectile dysfunction (ED) is defined as “the inability to achieve and / or maintain an erection sufficient to satisfy sexual activity” (Impotence. NIH Consensus Development Panel on Impotence, 1993) if these disorders have been observed for at least three months ... The term ED was proposed by the US National Institutes of Health to replace the old "impotence", which implies an overly categorical perception of the problem, causing disbelief in the prospect of treatment.
According to the WHO, after 21 years erectile dysfunction is detected in every 10th man, and after 60 years - every third man is not able to perform sexual intercourse at all. According to the calculations of J. B. MkKinlay (2000), about 150 million men in the world suffer from ED; this figure is expected to double over the next 25 years.
In a review published in 2003, A. Nicolosi cited the results of a standardized questionnaire survey of about 600 men aged 40 to 70 years in four countries of the world, according to which the frequency of ED was 15% in Brazil, 17% in Italy, and Malaysia - 22% and in Japan 34%. There are no epidemiological data on the prevalence of ED in Russia, however, the high injury rate among the male population, the significant prevalence of alcoholism, smoking of low-quality tobacco varieties and uncontrolled use of medications suggest a higher prevalence of ED compared to the industrial developed countries the world (G. S. Krotovsky, A. M. Zudin, 2003).
According to the results of the survey, 10 thousand men aged 17 to 70 years, conducted from April 12 to May 21, 2002 (P. Costa et al., 2003), only 22.2% of the surveyed men with ED seek help from a doctor, and only 36.9% of them receive treatment. Most of those surveyed did not consider ED as a disease, linking its occurrence to stress and fatigue. According to other studies, only a third of men consult a doctor (KS Fugl-Meyer, 1998 O. Kontula et al., 1995), and 75-88% of men with ED do not receive any treatment for this (F. Giuliano et al. , 2002, EJ Meuleman et al., 2001, KK Chew et al., 2000).
Thus, despite the high prevalence of ED, the patient demand for medical care is still quite low. Hence the ineffective (and sometimes unsafe) self-medication and further progression of the disease. Wide awareness not only of specialists directly involved in ED, but also of doctors of other specialties, namely therapists, endocrinologists, can play an important role in the primary diagnosis of ED. In addition, methods of treating ED cannot be considered in isolation from the general somatic condition of the patient, i.e., as an isolated urological problem, therefore, the involvement of doctors of other specialties can help to provide more qualified medical care to these patients.
Thus, ED is a widespread condition, and in the vast majority of cases, men do not seek medical help and do not receive adequate treatment. On the other hand, the general practitioner, to whom the patient first of all comes with all his problems, often has very vague ideas about the problem of ED and possible ways correction.
Erection: physiology and pathophysiology
An erection is an increase in the volume of the penis with a sharp increase in its elasticity, due to stretching and filling of the corpus cavernosum during sexual arousal. The phenomenon of erection consists of a complex chain of neurovascular changes in the cavernous tissue, the final link in which is the relaxation of the smooth muscle elements of the arteries, arterioles and sinusoids.
At the end of the last century, new data appeared on the physiology of erection, the causes of ED and, accordingly, new possibilities for its correction. According to modern concepts, during sexual stimulation, the parasympathetic nervous system is activated. The release of neurotransmitters, in particular nitric oxide, from the vascular endothelium of the corpora cavernosa leads to the accumulation of cyclic guanosine monophosphate (cGMP) in the cavernous tissue and relaxation of the smooth muscle cells of the walls of the vein arteries and cavernous bodies. Filling the lacunae with arterial blood causes compression of the venules and blocking the outflow of blood from the penis (veno-occlusive mechanism). The main components of an erection are shown in Figure 1.
Accordingly, the development of ED may be associated with insufficient vasodilation due to cGMP deficiency, poor vascular susceptibility to cGMP, lack of compression of the penile veins due to proliferation connective tissue; in addition, there may be a combination of the above reasons (D. Yu. Pushkar et al., 2002).
Thus, erection can be considered as a complex neurovascular phenomenon, in the origin of which sexual stimulation, the release of nitric oxide and the accumulation of cGMP in the cavernous tissue, relaxation and contraction of smooth muscle cells under the influence of PDE5 play a certain role.
Causes of erectile dysfunction
ED is usually divided into psychological (psychogenic), organic and mixed. If earlier various psychological problems were considered the main cause of ED (“if life is too business, the sexual function suffers”), now this opinion has changed. It has been shown that ED in 80% of cases is organic in nature and occurs as a complication of various somatic diseases (NIH Consensus Conference on Impotence, 1993). The main causes of ED are presented in Table 1. According to A. Nicolosi et al. (2003), there is an inverse relationship between the incidence of ED and the level of education, physical activity, and alcohol consumption.
Age in itself certainly has an impact on the usefulness and duration of erection in men. In older people, the blood flow rate, testosterone levels, the sensitivity of the nervous system and the elasticity of the vascular walls decrease, which accordingly affects the erection. However, such “natural” changes rarely lead to ED; and people not suffering chronic diseases internal organs are quite capable of living a full sexual life even at 80 years old. In the vast majority of men, the main cause of erectile dysfunction, as a rule, is precisely a somatic disease.
Almost all population studies on ED have found a relationship between its occurrence and arterial hypertension(AH), diabetes mellitus(DM) and atherosclerosis. So, according to E. Ricci et al. (2003), ED is six times more likely to occur in diabetes and three times more often in hypertension. Moreover, according to some authors, the detection of ED may indicate the presence of one of these diseases in a latent preclinical form in a patient (M. R. Nusbaum et al., 2002). According to M. K. Waiczak et al. (2002), out of 154 men who sought help for ED, 44% were diagnosed with hypertension and 23% with diabetes.
At atherosclerosis the walls of blood vessels lose their elasticity, their lumen narrows, there is a discrepancy between the organ's need for oxygen and the possibility of its delivery. At the same time, significant importance is attached to risk factors such as smoking, dyslipidemia, diabetes mellitus (R. A. Kloner, M. Speakman, 2002). Thus, E. Ricci et al. (2003) believe that 2/3 of patients with ED smoke, and the frequency of detection of hypercholesterolemia in them is twice as high as in patients without erectile dysfunction. Atherosclerotic changes in the penile bloodstream in about 40% of cases cause the development of ED in men over the age of 50. Often, various manifestations of atherosclerosis, such as coronary artery disease and ED, develop in parallel, since the risk factors for endothelial dysfunction of the coronary and penile blood vessels are the same. Therefore, it is no coincidence that cardiovascular diseases are significantly more common in patients with hypertension and ED than in patients with hypertension without sexual dysfunction (M. Burchardt et al., 2001). According to H. Solomon et al. (2003), among 174 men examined for ED, dyslipidemia was detected in 37%, uncontrolled hypertension - in 17%, exertional angina - in 6%. It is assumed that ED can serve as a marker of cardiovascular diseases, and its severity can be used to judge the progression of IHD (A. Greenstein et al., 1997, M. Kirby et al., 2001, H. Solomon, JW Man, G. Jackson, 2003). With a significant decrease in penile blood flow, according to Doppler ultrasound, some authors even recommend performing stress ECG tests before starting treatment for ED (Y. Kawanishi et al., 2001).
A number of studies have shown that against the background arterial hypertension ED is more common than in the general population. Thus, according to A. J. Cuellar De Leon et al. (2002), obtained as a result of a survey of 512 patients aged 30 to 86 years ( average age 63.4 years), ED occurs in 46.5% of patients with arterial hypertension. In a study by M. Burchardt et al. (2000), among 476 patients aged 34 to 75 years (average 62.2 years), 84.8% were sexually active and 68.3% had ED of varying severity (7.7% - moderate, 15.4 % - pronounced and 45.2% - severe), which significantly exceeds the population level. According to A. Roth et al. (2003), the incidence of ED among hypertensive patients is 46%.
Back in 1982, Jachuck et al. noted the relationship between sexual dysfunction and a deterioration in the quality of life in hypertensive patients treated with antihypertensive drugs, mainly diuretics, β-blockers or methyldopa (the latter drug, of course, is usually no longer used in the treatment of hypertension due to the high frequency of side effects). Approximately 78% of patients whose quality of life deteriorated significantly (as assessed by their wives) showed a decrease or lack of sexual interest. Collectively, studies conducted over 30 years have shown that 2.4% to 58% of men with hypertension experience one or more symptoms of sexual dysfunction of varying severity during treatment with antihypertensive drugs.
Especially often, the occurrence of ED is associated with the intake of thiazide diuretics and β-blockers (R. Fogari, A. Zoppi, 2002, H. Mickley, 2002, D. Ralph, T. McNicholas, 2000). So, according to S. Wassertheil-Smoller et al. (1991), obtained in a multicenter, randomized, placebo-controlled study TAIM, erection problems were detected in 11% of patients who received a β-blocker (atenolol) for six months, and in 28% of patients who received a thiazide diuretic (chlorthalidone ). D. T. Ko et al. (2002) conducted a meta-analysis and evaluated the safety of the use of β-blockers in hypertension and ischemic heart disease. The meta-analysis included the results of 15 studies (more than 35 thousand patients). It has been shown that the use of drugs in this group is associated with a small but statistically significant risk of sexual dysfunction (one additional case for every 199 patients treated with β-blockers during the year). First-generation β-blockers are more likely to cause ED than modern drugs, and their effect on the occurrence of ED does not depend on the degree of lipophilicity.
ED associated with hypertension or its treatment can reduce the quality of life of these patients and affect their adherence to therapy. For example, a five-year study by the Medical Research Council (MRC), which included 17 354 hypertensive patients, showed that sexual dysfunction is common reason refusal of patients from taking antihypertensive drugs. In this study, premature discontinuation of treatment for ED was observed significantly more frequently in patients taking a thiazide diuretic (p<0,001) либо β-аденоблокатор (p<0,001), по сравнению с пациентами, применявшими плацебо (12,6%, 6,3% и 1,3% на 1000 человеко-лет, соответственно). До 70% больных с АГ, у которых были выявлены побочные эффекты, не соблюдают режим приема антигипертензивных препаратов и 40—60% чаще прекращают лечение, по сравнению с пациентами, чье качество жизни не изменилось.
That is why practitioners need to be aware of the possibility of a variety of side effects in the genital area against the background of antihypertensive therapy and to conduct discussions with patients on this topic (Carlos M. Ferrario and Pavel Levy, 2001). In many cases, changing the drug regimen can help the patient overcome the negative sexual changes seen with some treatments. In addition, it is advisable to choose not only highly effective in terms of lowering blood pressure, but also not affecting the patient's quality of life, the tactics of antihypertensive therapy.
Not all classes of antihypertensive drugs are characterized by the same risk of developing sexual disorders. In particular, recent studies indicate that angiotensin II (AAII) antagonists may even improve erectile function in men with hypertension (R. Fogari et al., 1999, J. Caro et al., 2001, JL Llisterri et al., 2001). The beneficial effect of AAII on sexual function may be related to their ability to block angiotensin II receptors, which, as shown in the function of an experimental model of the penis, is able to stop spontaneous erection when applied exogenously.
Calcium antagonists also appear to at least not impair male sexual function. In any case, in the study by JE Marley (1989), which studied the tolerability of long-acting nifedipine (20 mg twice a day), four weeks after the start of therapy, the prevalence of ED decreased as in the group of patients who were previously treated with β-blockers and diuretics, and in the group of patients who have not previously received treatment.
With diabetes mellitus ED develops three times more often and 10-15 years earlier than in a healthy population. Its frequency, according to most studies, occurs in 50-75% of men with diabetes (A. Guay et al., 1998). In a study by G. De Berardis et al. (2002) involved 1460 patients with type 2 diabetes, observed in 114 clinics. Examination revealed ED in 34% of patients, periodic disorders of sexual function in 24%, and only 42% had no problems in their sexual life. In a survey of 1010 men with diabetes, followed for almost three years, ED was detected in 68 cases per 1000 patients per year (D. Fedele et al., 2001). The incidence of ED in men with diabetes increases with age and depends on the duration of the disease. If in patients under the age of 30, ED occurs in 9-15% of cases, at the age of 30 to 60 years - in more than 55% of cases, then over 70 years of age, ED affects up to 95% of patients with diabetes (Chu, Edelman, 2001) ... Apparently, precisely because of differences in age, ED occurs more often in type 2 diabetes than in type 1 diabetes (W. Alexander, 1999). The main causes of organic ED in diabetes mellitus are considered diabetic polyneuropathy, macro- and microangiopathy (A.T. Guay, 2002). It has been shown that ED in men with diabetes correlates, in addition to age, with the level of glycosylated hemoglobin (HbA1c), the presence of peripheral and autonomic neuropathy, and retinopathy (D. K. MkKulloch et al., 1980, J. H. Romeo et al., 2000).
Change can also play a role hormonal level- it was noted that 32-35% of men with ED have a decrease in testosterone levels (O.B. Laurent, A.S. Segal, 1999, A.S. Segal, 2002). This can be attributed to hypogonadism, obesity, and other metabolic disorders.
NS for chronic renal failure more than 50% of patients complain of sexual dysfunction (W. R. Procci, et al, 1986). Conducted by S. R. Holdsworth et al. (1978) a study of nocturnal erections in these individuals showed that ED is most often organic in nature and that dialysis improves sexual function, but does not normalize it. Renal transplant is more effective if it functions normally (W. L. Diemont et al., 2000). In a study by T. E. Steele et al. (1996) among 68 patients with chronic renal failure who received peritoneal dialysis, 63% did not have sexual contacts, in 19% their frequency did not exceed twice a month, and only 18% had sexual contacts more than twice a month. As shown by psychological testing, in patients who had no sexual contacts, the level of anxiety was higher, and the quality of life was lower than in patients with preserved sexual activity.
For chronic obstructive pulmonary disease Our own studies have shown that ED occurs in 12 out of 20 men with chronic obstructive bronchitis and bronchial asthma. The literature mentions cases of ED in patients with obesity, duodenal ulcer, especially associated with Helicobacter pylori, steatohepatitis, urinary infection, etc., however, these studies are currently few.
In men suffering depression, the likelihood of developing ED ranges from 25% in mild depression to almost 90% in severe depression (H. A. Feldman et al., 1994). ED can be triggered by severe stress, such as the tragic death of loved ones. More often, however, there is a psychogenic variant associated with a man's disbelief in his own sexual usefulness - the so-called situational ED. It is caused by self-doubt, fear of failure, "shameful" failure, because of which a man does not dare to enter into an intimate relationship at all. Psychological testing revealed that men who are prone to overt or latent outbursts of anger are more likely than others to suffer from moderate or even complete ED. It should be borne in mind that the presence of risk factors for organic ED does not exclude the likelihood of developing psychological ED (E.V. Bondareva, 2002).
Thus, ED is 80% organic in nature and arises as a complication of somatic diseases - hypertension, atherosclerosis, diabetes mellitus, chronic renal failure, etc. Various mechanisms can participate in the development of ED: neurogenic, vascular, and the effects of drugs. At the same time, the inverse relationship between the frequency of occurrence of ED and the level of education, physical activity, and alcohol consumption is important.
Diagnosis of erectile dysfunction
Diagnosis of ED is based on history, physical examination, instrumental and laboratory research (see).
The collection of information facilitates the use of tailored questionnaires for patients with ED. The use of these questionnaires allows not only to smooth out the feeling of awkwardness in a conversation with a shy patient, but also to save the doctor's time. In clinical studies, the Brief Male Sexual Function Inventory (BMSFI), Sexual Encounter Profile (SEP), and Global Assessment Question (GAQ) are most often used to assess sexual function in men.
In Russia, the ICF Scale (Male Copulative Function), proposed by O.B. Laurent and A.S. Segal (1998), is often used and is focused more on the analysis of sexual dysfunctions of organic rather than mental genesis. The use of the ICF scale is possible only if certain conditions are met. These include: a man has a permanent sexual partner, a friendly relationship with her and acceptable conditions for sexual life. The content of the questionnaires is given in.
Routine laboratory examination includes the determination of testosterone and blood glucose levels; according to indications determine the level of blood lipids, prolactin, PSA (A. G. Jardin et al., 2000). Several studies have shown the importance of measuring blood hormone levels in men with ED. So, according to J. Buvat et al. (1997), among 1022 men with ED, 4% of those under 50 and 9% over 50 had a consistently low serum testosterone concentration; many of them have benefited from testosterone treatment. In another study of 422 men with ED, hormonal disorders were detected in 29% of cases, including hypogonadism - in 19%, hyperprolactinemia - in 4%, hypo- or hyperthyroidism - in 6% (M. F. Stag et al., 1983).
Further examination is indicated for persons with primary ED to exclude its organic nature; young men with a history of trauma to the perineum or pelvic organs (due to the possible need for surgical treatment); at the request of the patient or his partner; during medical examination (E. Wespes et al., 2002).
The next screening study may be monitoring of nocturnal spontaneous erections. It was found that in healthy men during the night in the phase of REM sleep, there are four to six episodes of erections, lasting 10-15 minutes. The total duration of spontaneous erections is 1.5 hours, or 20% of the sleep time. Men with ED show a decrease in the quality and quantity of spontaneous erections during nighttime sleep. This fact made it possible to use monitoring for the differential diagnosis of organic and psychogenic forms of sexual disorders (see). A registered episode of erection with a rigidity of 60% lasting more than 10 minutes indicates functional erectile dysfunction (E. J. Meuleman, W. L. Diemont, 1995). It is believed that monitoring of nocturnal spontaneous erections makes it possible to quantitatively and qualitatively assess the erectile function of men better than any other method (J. Chen, M. F. Godschalk, 1999; D. Udelson et al., 1999).
Doppler ultrasound(USDG) of the arteries of the penis allows to assess microcirculation, and its conduction in B-mode - to reveal structural changes in cavernous fibrosis and Peyronie's disease (Klinger et al., 1999). However, the results of the study using the duplex method turn out to be much more complete than with the separate use of modes B and D. In addition, the quality of the study largely depends on the technical perfection of the apparatus on which it is carried out (Mancini et al., 2000; Cornud et al., 2000). Doppler ultrasonography of the penile arteries is more informative if it is performed at rest and erection with subsequent comparison of the results (Mellinger et al., 1999; Roy et al., 2000; Chen et al., 2000), which is achieved using functional tests - visual stimulation (erotic film) or drug (viagra) test (Arslan et al., 2001).
The main quantitative indicators are the maximum (peak) systolic velocity (PSV) and end diastolic velocity (EDV). On the basis of absolute indicators according to standard formulas, the relative ones are calculated - the resistance index (RI) and the pulsation index (PI). Usually, PSV equal to 30-35 cm / s is taken as the norm (Migaleddu et al., 2000), less often the lower limit of the norm begins to be counted from 25 cm / s (Mancini et al., 1996; Furst et al., 1999). After pharmacological stimulation, the highest value for a given patient is usually achieved within 5-10 minutes. In this case, the acceleration should exceed 400 cm / s2 (Valji et al., 1993), and the acceleration time should be less than 0.1 s (Patel et al., 1993).
One of the diagnostic techniques is the Viagra test in combination with visual stimulation against the background of erectile monitoring (A. Erbagci et al., 2002) and assessment of penile hemodynamics by ultrasound scanning (E.B. Mazo et al., 2002). The advantages of the test include non-invasiveness and the absence of the threat of priapism; to the disadvantages - the need for visual stimulation, which does not allow standardizing the method - different men need different stimuli (G. S. Krotovsky, A. M. Zudin, 2003). The new PDE5 inhibitor tadalafil (Cialis) has the same mechanism of action and is characterized by a fairly rapid onset of effect. Already at the 16th minute, 32% of men achieve an erection with sexual stimulation. Another feature of the drug - the duration of the effect is 36 hours - gives the patient the opportunity not only to be convinced of the effectiveness of the drug during the diagnostic procedure, but also then to have sexual intercourse in natural conditions for him.
A test with intracavernous administration of vasoactive drugs (usually alprostadil, an analogue of prostaglandin E) reveals vasculogenic ED. With normal arterial and veno-occlusive hemodynamics, 10 minutes after injection, a pronounced erection occurs, which persists for 30 minutes or more (E. J. Meuleman, W. L. Diemont, 1995).
According to the indications, other studies are also performed, namely:
- cavernosometry (determination of the volumetric velocity of the physiological solution pumped into the cavernous bodies, which is necessary for the occurrence of an erection) is the main test that directly evaluates the degree of violation of the elasticity of the sinusoidal system and its closure ability;
- cavernosography (demonstrates venous vessels, through which blood is mainly discharged from the corpora cavernosa);
- radioisotope phallic scintigraphy (allows you to assess the qualitative and quantitative indicators of regional hemodynamics in the corpora cavernosa of the penis);
- neurophysiological studies, in particular, the determination of the bulbocavernous reflex in patients with diabetes, with spinal cord injury.
Thus, modern diagnostic methods, using a sufficient volume of research, make it possible to determine the cause of erectile dysfunction with high accuracy. This is primarily necessary for the implementation of the pathogenetic approach to the choice of treatment.
ED treatment
Not only among patients, but also, unfortunately, some doctors have an idea of the inevitability of the extinction of sexual function in old age and the impossibility of influencing this process. However, with adequately selected treatment, 95% of patients can be helped. At the first stage, after clarifying the presence of somatic pathology, the attending physician decides on the correction and treatment of this ailment. So, for example, in patients with hypertension and diabetes, it is necessary to select an effective and safe antihypertensive or antihypertensive therapy, in COPD - the abolition of theophylline drugs, adrenomimetics and the appointment of inhaled anti-inflammatory therapy, in peptic ulcer disease - the replacement of H2-blockers of histamine with proton pump inhibitors, in chronic renal failure - enhancing dialysis and correcting anemia.
The most effective and convenient method of treating both psychogenic and organic ED is the use of phosphodiesterase type 5 inhibitors (PDE5). During sexual stimulation, due to the activation of the nervous system and the release of nitric oxide (NO), cyclic guanosine monophosphate (cGMP) accumulates in vascular smooth muscle cells. As described earlier, it is cGMP that triggers a cascade of biochemical reactions leading to the onset and maintenance of an erection. Normally, its concentration decreases with the cessation of sexual stimulation due to destruction by phosphodiesterase-5. In ED, there is a deficiency of cGMP due to various pathogenetic factors, and its destruction by PDE5 leads to insufficient erection or lack thereof. PDE5 inhibitors do not have a direct relaxing effect on the corpora cavernosa, but enhance the relaxing effect of nitric oxide by inhibiting PDE5 and increasing the concentration of cGMP during sexual arousal.
In the domestic literature there are fairly detailed publications on the use of sildenafil citrate (Viagra). Recently, another drug from the group of PDE5 inhibitors has become available for clinical practice in Russia - tadalafil (Cialis, Lilly / ICOS), which differs from sildenafil in chemical structure, selectivity, pharmacokinetic profile and, accordingly, in clinical action.
The pharmacokinetic profiles of sildenafil and tadalafil differ significantly: the half-life of tadalafil significantly exceeds the corresponding values of sildenafil. The clinical effect of tadalafil develops in one third of patients after 16 minutes and in the vast majority of patients (79%) persists for 36 hours after taking the drug (I. Eardley et al., 2002, H. Padma-Nathan et al., 2001). Due to the long-term effects of the drug, the couple can more freely choose the time of intimacy. For example, after taking a pill on Friday evening, sexual relations are possible at any time until Sunday morning, which frees you from the need to clearly plan your intimate life. The simultaneous intake of fatty foods and alcohol does not affect the concentration of the drug in the blood serum (B. Patterson et al., 2001). This is practically important, since it makes it possible not to change the patient's usual lifestyle.
Despite the fact that tadalafil has only recently become available in general practice, it is nevertheless fairly well studied. Currently, more than 90 clinical trials have been conducted (including long-term ones, lasting up to two years), during which the drug has unequivocally proved its effectiveness and safety. So, in order to assess the clinical efficacy and safety of tadalafil B. Brock et al. (2002) conducted an integrative analysis of five randomized, double-blind, placebo-controlled, parallel-group studies. These studies were carried out in 1999-2001. in 74 medical centers and covered 1112 men aged 22 to 82 years with severe or severe ED (in 61% of cases - organic, in 9% - psychogenic and 31% - mixed). Patients received tadalafil in a daily dose of 2.5 mg, 5 mg, 10 mg, 20 mg or placebo without restriction of food and alcohol consumption. The IIEF (International Index of Erectile Function), SEP (Sexual Relationship Profile) and GAQ (General Impression Question) questionnaires were used to assess the effectiveness of the drug. The main results of the study are presented in Figure 2.
Among patients who received tadalafil at a dose of 20 mg per day, normal erectile function (score 26 or more in the IIEF questionnaire) was achieved in 59% of men compared with 11% in the control group. On the background of treatment with tadalafil at a dose of 20 mg per day, the absolute proportion of successfully completed attempts at intercourse was 75%, compared with 32% in the placebo group (SEP). At the end of treatment, 81% of men who received tadalafil at a dose of 20 mg per day, and only 35% of men in the placebo group, reported improved erections (GAQ questionnaire). The efficacy of the drug was the same in young patients and in those over 65 years old and did not depend on the etiology of ED. When assessing the effect of tadalafil on the success of intercourse completion depending on the time after taking 20 mg of the drug (according to the questionnaire using the SEP questionnaire), it turned out that a total of 73 to 80% of sexual intercourse attempts made between 30 minutes and 36 h were successful.
Given the high prevalence of ED among diabetic patients, the efficacy and safety of tadalafil at a dose of 10 and 20 mg was evaluated in a 12-week, randomized, placebo-controlled study that included 216 patients with type I or II diabetes and ED (I. Saenz de Tejada et al., 2002). According to the questionnaire survey using the IIEF questionnaire, the increase in the average score reflecting erectile function during therapy with tadalafil at doses of 10 and 20 mg was 6.4 and 7.3, respectively, after 12 weeks, compared to 0.1 in the placebo group. The percentage of patients who reported success in achieving and maintaining an erection (SEP) and noted an improvement in erection (GAQ) was also significantly higher with tadalafil therapy than in the placebo group.
Among the undesirable phenomena that arose while taking tadalafil, the most common were headache and dyspepsia, less often back pain, nasal congestion, myalgia and flushing of the face; no clinically significant visual impairments were observed. Side effects, as a rule, were not severe and decreased with continued treatment; the withdrawal rate due to adverse events was 1.6% during therapy with tadalafil at a dose of 10 mg per day, 3.1% during therapy with the drug at a dose of 20 mg per day, and 1.3% in the placebo group. In a study by W. J. Hellstrom et al. (2002) daily intake of tadalafil at a dose of 10 or 20 mg per day for six months did not adversely affect human spermatogenesis. An open-label two-year study of 1173 patients (mean age 57 years) also showed good tolerance to tadalafil (F. Montorsi et al., 2001).
The main concerns associated with the use of PDE5 inhibitors are due to their potential vasodilating effect, therefore, in a number of phase III studies, the cardiovascular effects of tadalafil were specifically studied in healthy volunteers and in patients with exertional angina and hypertension. In healthy individuals, taking tadalafil at a dose of 10 and 20 mg did not cause a statistically insignificant decrease in blood pressure in the standing position; in general, the effect of the drug on hemodynamic parameters did not differ from the effect of placebo. Tadalafil does not lengthen the QT interval, does not cause disturbances in atrioventricular conduction and heart rhythm. The frequency of cardiovascular side effects of tadalafil is comparable to the corresponding indicators in the placebo group (see); its use is safe in patients receiving antihypertensive therapy. In more than 1200 patients, the incidence of myocardial infarction during therapy with tadalafil was 0.39 per 100 person-years - versus 1.1, in persons receiving placebo, and was comparable to the corresponding indicator in the age-standardized male population (0.6 ) (JT Emmick et al., 2002).
The safety of the combination of tadalafil with amlodipine at a dose of 5 mg / day, metoprolol at a dose of 25-200 mg / day, enalapril at a dose of 10-20 mg / day, indapamide at a dose of 2.5 mg / day, losartan at a dose of 25-50 mg has been shown. / day However, tadalafil, like sildenafil, cannot be prescribed in combination with nitrates, since in a certain group of patients the combined use of these drugs leads to the development of severe arterial hypotension (R. A. Kloner, M. I. Mitchell et al., 2002). With the development of an attack of angina pectoris during therapy with PDE5 inhibitors, the use of nitroglycerin is categorically contraindicated, the use of any form of nitrates is possible 48 hours after the last use of tadalafil. With caution, drugs in this group are used in the presence of anatomical deformities of the penis and diseases that contribute to the occurrence of priapism (for example, sickle cell anemia, leukemia). Thus, drug therapy with PDE5 inhibitors is a simple, effective, and fairly safe method of treating ED.
In conclusion, I would like to emphasize that ED develops, as a rule, against the background of chronic diseases, therefore, the role of general practitioners is difficult to overestimate in the identification and treatment of this condition. The emergence of new effective, safe and easy-to-use drugs for the treatment of ED makes it possible to successfully solve this problem in the context of general therapeutic practice.
A. L. Vertkin, Doctor of Medical Sciences, Professor
D. Yu. Pushkar, Doctor of Medical Sciences, Professor
A. V. Topolyansky, Candidate of Medical Sciences, Associate Professor
A.S.Segal, Doctor of Medical Sciences, Professor
MGMSU, Moscow
Accidentally came across this drug in the list of reviews. Legends and myths have been circulating about Viagra for a long time, and no matter how much they write and talk about its side effects, men still buy and take it, and even without consulting a doctor, and more often on the sly, so that no one knows at all. I have an illustrative case with a close relative.
I remember Eugene Onegin: "My uncle had the most honest rules when he got seriously ill ..." We got the same situation. Mom called and said to urgently go to the hospital, as my uncle was in intensive care, presumably with a stroke, and only my husband and I were among the relatives within a radius of 200 km. Naturally, let's go. Auntie is all in tears, the mood for the worst, does not come to her senses. Two days of aunt's tantrums, resuscitation, intensive therapy, and as a result - a man at 52 has the right side of his face paralyzed, his right hand does not work, and his right leg is difficult to control. Speech is slurred, as the tongue and facial muscles also refuse to work. Now disability.
And the background, as it turned out, was banal. According to his aunt, from a very young age, the uncle had a high sexual potential, could be active every day, changed several mistresses during their family life. And after 50 years, the strength began to weaken. And since the person was so accustomed to his "victories" that he did not want to put up with the situation, and they agreed with his wife, two years after the beginning of the problems, they decided to buy Viagra. Moreover, it was an independent decision, without the participation of a doctor. And the very first pill of the stimulant led to the fact that twenty minutes later the man first rushed blood in his face, then it became difficult to breathe, and in the end he simply fell down at his aunt's feet, and did not have time to reach the bed. The tomography showed a unilateral cerebral hemorrhage. And the corresponding consequences, which they are now trying to rehabilitate, although whether there is hope is a moot point. Thank God that he remained alive.
I do not want to dissuade anyone or scold these Viagra pills. The decision in any case remains with the one who is going to drink them. But first, study the contraindications.
And if you still dare to drink them, then you need to act on the points. Point one: in no case should Viagra be taken by men who have problems with the heart or blood vessels. Point two: be sure to consult a doctor (although it should be P1). Point three: most men do not even suspect that they have or may have problems with the heart and blood vessels, therefore, in order to exclude point one, point two must be completed. In general, I will tell you as a girl - happiness is not in sex :) Be healthy.
regarding the processing of personal data of website visitors
1. General Provisions
1.1. This Policy regarding the processing of personal data (hereinafter referred to as the "Policy") has been prepared in accordance with clause 2, part 1 of Art. 18.1 of the Federal Law of the Russian Federation "On Personal Data" No. 152-FZ of July 27, 2006 (hereinafter - the "Law") and determines the position of the legal entity LLC Alargo (PSRN: 1117847317653, TIN: 7814507900, registration address: 197342, St. St. Petersburg, Serdobolskaya street 64, building 1, letter A, office 514) and / or its affiliates, (hereinafter - the "Company") in the field of processing and protection of personal data (hereinafter - the "Data"), respect for the rights and freedoms of every person and, in particular, the right to privacy, personal and family secrets.
2. Scope
2.1. This Policy applies to the Data received both before and after the entry into force of this Policy.
2.2. Understanding the importance and value of the Data, as well as taking care of the observance of the constitutional rights of citizens of the Russian Federation and citizens of other states, the Company ensures reliable protection of the Data.
3. Definitions
3.1. Data is understood as any information relating directly or indirectly to a specific or identifiable natural person (citizen), i.e. such information, in particular, includes: surname, name, patronymic, registration / mailing address, e-mail, phone number, location, photo, ip address.
3.2. Data processing means any action (operation) or a set of actions (operations) with Data performed using automation tools and / or without using such tools. Such actions (operations) include: collection, recording, systematization, accumulation, storage, clarification (update, change), extraction, use, transfer (distribution, provision, access), depersonalization, blocking, deletion, destruction of Data.
3.3. Data security means the Data security against unauthorized and / or unauthorized access to them, destruction, alteration, blocking, copying, provision, dissemination of Data, as well as against other illegal actions in relation to the Data.
4. Legal bases and purposes of data processing
4.1. The processing and security of Data in the Company is carried out in accordance with the requirements of the Constitution of the Russian Federation, the Law, the Labor Code of the Russian Federation, bylaws, and other federal laws of the Russian Federation that determine the cases and features of the processing of Data, guidelines and methodological documents of the FSTEC of Russia and the FSB of Russia.
4.2. The subjects of the Data processed by the Company are:
- candidates for vacant positions, including candidates filling out a candidate's questionnaire on the Company's Internet resource: “Extender24”
- employees of the Company, relatives of employees of the Company, within the limits determined by the legislation of the Russian Federation, if information about them is provided by the employee;
- persons who are members of the management bodies of the Company and are not employees; individuals with whom the Company concludes contracts of a civil nature;
- clients - consumers, incl. visitors to the site https: // site owned by the Company, including for the purpose of placing an order on the Site https: // site with subsequent delivery to the client, recipients of services ;,
4.3. The company processes the Data of subjects for the following purposes:
- implementation of the functions, powers and duties assigned to the Company by the legislation of the Russian Federation in accordance with federal laws, including, but not limited to: the Civil Code of the Russian Federation, the Tax Code of the Russian Federation, the Labor Code of the Russian Federation, the Family Code of the Russian Federation, the Federal Law of 01.04 .1996 No. 27-FZ "On individual (personified) accounting in the compulsory pension insurance system", Federal Law of 27.07.2006, No. 152-FZ "On personal data", Federal Law of 28.03.1998, No. 53 -FZ "On military duty and military service", Federal Law of February 26, 1997, No. 31-FZ "On mobilization training and mobilization in the Russian Federation", Federal Law of February 8, 1998, No. 14-FZ "On societies with limited liability ", Federal Law of 07.02.1992 No. 2300-1" On Protection of Consumer Rights ", Federal Law of 21.11.1996, No. 129-FZ" On Accounting ", F Federal Law of November 29, 2010 No. 326-FZ "On Compulsory Health Insurance in the Russian Federation",
- Employees in order to comply with the labor, tax and pension laws of the Russian Federation, namely:
1. assistance to employees in employment, training and promotion;
2. calculation and calculation of wages;
3. organization of business trips (business trips) of employees;
4. issuing powers of attorney (including for representing the interests of the Company to third parties);
5. ensuring the personal safety of employees; o control the quantity and quality of work performed;
6. ensuring the safety of property;
7. compliance with the access control in the premises of the Company; - Applicants for vacant positions in order to:
1. making a decision on the possibility of concluding an employment contract with persons applying for open vacancies; - Persons who are members of the Company's governing bodies, who are not employees, in order to:
1. fulfillment of the requirements stipulated by the legislation, incl. mandatory disclosure of information, audit, verification of the possibility of making transactions, including interested-party transactions and / or major transactions. - Clients - consumers in order to:
1. providing information on goods / services, ongoing promotions and special offers;
2. analysis of the quality of the service provided by the Company and improvement of the quality of customer service of the Company;
3. informing about the status of the order;
4. performance of the contract, incl. sales contracts, incl. concluded remotely on the Site, paid provision of services; provision of services, as well as accounting for services rendered to consumers for the implementation of mutual settlements;
5. delivery of the ordered goods to the client who made an order on the Site, return of the goods.
5. Principles and conditions for data processing.
5.1. When processing Data, the Company adheres to the following principles: Data processing is carried out on a legal and fair basis; The Data is not disclosed to third parties and is not disseminated without the consent of the Data subject, except for cases requiring the disclosure of Data at the request of authorized state bodies, legal proceedings; determination of specific legitimate purposes before the start of processing (including collection) of the Data; only those Data are collected that are necessary and sufficient for the stated purpose of processing; unification of databases containing Data, the processing of which is carried out for purposes incompatible with each other is not allowed; the processing of the Data is limited to the achievement of specific, predetermined and legitimate purposes; The processed Data are subject to destruction or depersonalization upon achievement of the processing goals or in case of loss of the need to achieve these goals, unless otherwise provided by federal law.
5.2. The Company may include the Data of subjects in publicly available sources of Data, while the Company takes the subject's written consent to the processing of his Data, or by expressing consent through the site form (checkbox), by clicking which the subject of personal data expresses his consent.
5.3. The Company does not process Data related to race, nationality, political views, religious, philosophical and other beliefs, intimate life, membership in public associations, including trade unions.
5.4. The Company may process data on the health status of the Data subject in the following cases: 1) in accordance with the legislation on state social assistance, labor legislation, the legislation of the Russian Federation on pensions for state pensions, on labor pensions; 2) to protect the life, health or other vital interests of the employee or to protect the life, health or other vital interests of other persons and obtaining the consent of the Data subject is impossible; 3) to establish or exercise the rights of an employee or third parties, as well as in connection with the administration of justice; 4) in accordance with the legislation on compulsory types of insurance, with insurance legislation.
5.5. Biometric Data (information that characterizes the physiological and biological characteristics of a person, on the basis of which it is possible to establish his identity and which is used by the operator to establish the identity of the Data subject) are not processed in the Company.
5.6. The Company does not carry out cross-border transfers of Data.
5.7. In the cases established by the legislation of the Russian Federation, the Company has the right to transfer Data to third parties (the federal tax service, the state pension fund and other state bodies) in the cases provided for by the legislation of the Russian Federation.
5.8. The transfer of personal data to third parties can be carried out only in cases established by the legislation of the Russian Federation, an agreement with the participation of the User or with his consent. With this Consent, the User confirms his consent to provide the Company with the User's personal data to the following partners and bodies, and also agrees to the processing of the User's personal data by these partners (bodies) in the volumes, methods and for the period specified in this consent, but no more than required to ensure the purposes of processing indicated on the website at the Internet address https: // website, to perform certain functions of the Company, namely:
- LLC "LOGNEX" (Address: 121205, Moscow, Skolkovo Territory of the Innovation Center, Bolshoi Blvd., 42, building 1, room 1617, INN: 7736570901) - for processing personal data (name, address, phone, e-mail) of this Policy, for the following purposes: for warehouse accounting
- LLC "Index-Express" (Address: 192007, St. Petersburg, Kurskaya st., House number 27, letter A, room 4N, INN: 7816581338) - for the processing of personal data (name, address, phone, email) of this Policies for the following purposes: for order delivery using the site at the address on the Internet https: // site.
- "EMS Russian Post" branch of the Federal State Unitary Enterprise "Russian Post" (Address: 195009, St. Petersburg, Komsomola st., 37, building 3, letter A, INN: 7724261610) - for the processing of personal data (name , address, telephone) of this Policy, for the following purposes: for order delivery using the site at the address on the Internet https: // site.
- LLC "Network of automated points of delivery" (Address: 109316, Moscow, Volgogradsky avenue, 42, building 23, INN: 7723763977) - for the processing of personal data (name, address, phone, email) of this Policies for the following purposes: for order delivery using the site at the address on the Internet https: // site.
- IE Pavlov Vyacheslav Sergeevich (Address: 410062, Saratov, Motornaya st., 6, apt. 36, INN: 645399265598) - for the processing of personal data (name, phone, e-mail) of this Policy, for the following purposes: for tracking shipments by courier companies using the site at the address on the Internet https: // site.
5.9. Persons who process Data on the basis of an agreement concluded with the Company (instructions of the operator) undertake to comply with the principles and rules for the processing and protection of Data provided for by the Law. For each third party, the agreement defines a list of actions (operations) with the Data that will be performed by a third party processing the Data, the purposes of processing, the obligation of such a person to maintain confidentiality and ensure the security of the Data during their processing is established, the requirements for the protection of the processed Data are specified in accordance with with the Law.
5.10. In order to comply with the requirements of the current legislation of the Russian Federation and its contractual obligations, the Data processing in the Company is carried out both with and without the use of automation tools. The set of processing operations includes the collection, recording, systematization, accumulation, storage, clarification (update, change), extraction, use, transfer (provision, access), depersonalization, blocking, deletion, destruction of Data.
5.11. The Company prohibits making decisions based solely on automated processing of the Data that generate legal consequences in relation to the Data subject or otherwise affect his rights and legitimate interests, except as otherwise provided by the legislation of the Russian Federation.
6. Rights and obligations of data subjects, as well as the Company in terms of data processing
6.1. The subject whose Data is processed by the Company has the right:
- receive from the Company:
- confirmation of the fact of processing the Data and information about the availability of Data related to the relevant Data subject;
- information on the legal grounds and purposes of the Data processing;
- information about the methods of data processing used by the Company;
- information about the name and location of the Company;
- information about persons (with the exception of employees of the Company) who have access to the Data or to whom the Data may be disclosed on the basis of an agreement with the Company or on the basis of federal law;
- a list of processed Data related to the Data subject, and information about the source of their receipt, unless another procedure for providing such Data is provided for by federal law;
- information about the terms of data processing, including the terms of their storage;
- information on the procedure for exercising by the Data subject of the rights provided for by the Law;
- name (full name) and address of the person processing the Data on behalf of the Company;
- other information provided for by the Law or other regulatory legal acts of the Russian Federation;
- demand from the Company:
- clarification of their Data, their blocking or destruction in the event that the Data is incomplete, outdated, inaccurate, illegally obtained or is not necessary for the stated purpose of processing;
- revoke your consent to the processing of Data at any time; demand the elimination of illegal actions of the Company in relation to its Data;
- appeal against the actions or inaction of the Company to the Federal Service for Supervision of Communications, Information Technology and Mass Media (Roskomnadzor) or in court if the Data subject believes that the Company is processing his Data in violation of the requirements of the Law or otherwise violates his rights and freedom;
- to protect their rights and legitimate interests, including compensation for damages and / or compensation for moral damage in court.
6.2. In the process of processing the Data, the Company is obliged to:
- provide the Data subject, upon his request, with information regarding the processing of his personal data, or legally provide a refusal within thirty days from the date of receipt of the request from the Data subject or his representative;
- explain to the Data subject the legal consequences of refusing to provide Data if the provision of Data is mandatory in accordance with federal law;
- prior to the start of the processing of the Data (if the Data was not received from the Data subject), provide the Data subject with the following information, with the exception of cases provided for in part 4 of Article 18 of the Law:
1) the name or surname, name, patronymic and address of the Company or its representative;
2) the purpose of the Data processing and its legal basis;
3) intended users of the Data;
4) the rights of Data subjects established by the Law;
5) the source of obtaining the Data. - take the necessary legal, organizational and technical measures or ensure their adoption to protect the Data from unauthorized or accidental access to them, destruction, alteration, blocking, copying, provision, dissemination of Data, as well as from other illegal actions in relation to the Data;
- publish on the Internet and provide unrestricted access using the Internet to the document defining its policy in relation to the processing of Data, to information about the implemented data protection requirements;
- provide data subjects and / or their representatives free of charge the opportunity to familiarize themselves with the Data when submitting an appropriate request within 30 days from the date of receipt of such a request;
- to block unlawfully processed Data related to the Data subject, or to ensure their blocking (if the Data processing is carried out by another person acting on behalf of the Company) from the moment of contacting or receiving a request for a verification period, in case of unlawful processing of Data when the Data subject or his a representative or at the request of the Data subject or his representative or an authorized body for the protection of the rights of personal data subjects;
- clarify the Data or ensure their clarification (if the Data processing is carried out by another person acting on behalf of the Company) within 7 working days from the date of submission of the information and remove the blocking of the Data, in case of confirmation of the fact of inaccuracy of the Data based on the information provided by the Data subject or his representative;
- stop unlawful processing of the Data or ensure the termination of unlawful processing of Data by a person acting on behalf of the Company, in the event of unlawful processing of Data carried out by the Company or a person acting on the basis of an agreement with the Company, within a period not exceeding 3 working days from the date of this identification;
- stop processing the Data or ensure its termination (if the processing of the Data is carried out by another person acting under an agreement with the Company) and destroy the Data or ensure their destruction (if the processing of the Data is carried out by another person acting under an agreement with the Company) to achieve the purpose of processing the Data, unless otherwise is not provided for by an agreement to which the Data subject is a party, beneficiary or guarantor, if the purpose of the Data processing is achieved;
- stop processing the Data or ensure its termination and destroy the Data or ensure their destruction if the Data subject withdraws consent to the processing of the Data, if the Company is not entitled to process the Data without the consent of the Data subject;
- keep a register of applications of PD subjects, in which the requests of the Data subjects for receiving the Data, as well as the facts of providing the Data on these requests, should be recorded.
7. Requirements for data protection
7.1. When processing the Data, the Company takes the necessary legal, organizational and technical measures to protect the Data from unauthorized and / or unauthorized access to them, destruction, alteration, blocking, copying, provision, dissemination of Data, as well as from other illegal actions in relation to the Data.
7.2. Such measures in accordance with the Law, in particular, include:
- appointment of a person responsible for organizing the processing of the Data and a person responsible for ensuring the security of the Data;
- development and approval of local acts on the processing and protection of Data;
- application of legal, organizational and technical measures to ensure the security of the Data:
· Identification of threats to the security of the Data during their processing in personal data information systems;
· Application of organizational and technical measures to ensure the security of the Data during their processing in personal data information systems, necessary to meet the requirements for data protection, the implementation of which is ensured by the Data security levels established by the Government of the Russian Federation;
· Application of the procedure for assessing the conformity of information protection means that have passed in accordance with the established procedure;
· Assessment of the effectiveness of measures taken to ensure the security of the Data prior to the commissioning of the personal data information system;
· Accounting of machine data carriers, if the storage of the Data is carried out on machine carriers;
· Detection of facts of unauthorized access to the Data and taking measures to prevent similar incidents in the future;
· Recovery of Data, modified or destroyed due to unauthorized access to them;
Establishing rules for accessing the Data processed in the personal data information system, as well as ensuring registration and accounting of all actions performed with the Data in the personal data information system. - control over the measures taken to ensure the security of the Data and the level of security of information systems of personal data;
- assessment of harm that may be caused to Data subjects in case of violation of the requirements of the Law, the ratio of this harm and the measures taken by the Company aimed at ensuring the fulfillment of the obligations provided for by the Law;
- compliance with the conditions that exclude unauthorized access to material data carriers and ensure the safety of the Data;
- familiarization of the Company's employees who directly process the Data with the provisions of the legislation of the Russian Federation on Data, including the requirements for Data protection, local acts on the processing and protection of Data, and training of the Company's employees.
8. Terms of data processing (storage)
8.1. The terms of processing (storing) the Data are determined based on the purposes of processing the Data, in accordance with the term of the agreement with the Data subject, the requirements of federal laws, the requirements of the Data operators on whose behalf the Company processes the Data, the basic rules for the archives of organizations, and the limitation period.
8.2. Data, the processing (storage) period of which has expired, must be destroyed, unless otherwise provided by federal law. Storage of the Data after the termination of their processing is allowed only after their depersonalization.
9. The procedure for obtaining clarifications on the processing of Data
9.1. Persons whose Data is processed by the Company can receive clarifications on the processing of their Data by contacting the Company personally or by sending a corresponding written request to the address of the Company's location: 197342, St. Petersburg, st. Serdobolskaya d.64, building 1, letter A, office 514.
9.2. In the case of sending an official request to the Company, the text of the request must indicate:
- surname, name, patronymic of the Data subject or his representative;
- number of the main identity document of the Data subject or his representative, information on the date of issue of the specified document and the issuing authority;
- information confirming that the Data subject has a relationship with the Company; information for feedback in order to send the Company a response to the request;
- the signature of the Data subject (or his representative). If the request is sent in electronic form, then it must be executed in the form of an electronic document and signed with an electronic signature in accordance with the legislation of the Russian Federation.
10. Features of processing and protection of Data collected by the Company using the Internet
10.1. The Company processes the Data received from users of the Site, including the Data of Candidates for vacant positions from the resource: https: // site (hereinafter collectively - the Site), as well as received by the phone of the Company: 88005550486, to the email address of the Company: [email protected], through the Company's feedback form located at:.
10.2. Data collection
There are two main ways in which the Company obtains Data via the Internet:
10.2.1. Provision of Data
Provision of Data (self-entry of data):
- surname
- patronymic
- registration / mailing address
- phone number
- the photo
10.2.2. Data Subjects by way of receipt at the Company's telephone number: 88005550486, at the Company's e-mail address: [email protected], through the Company's feedback form located at:.
10.3. Automatically collected information
The company may collect and process information that is not personal data:
- locating
- ip address
- information about the interests of users on the Site based on the entered search queries of the users of the Site about the goods sold and offered for sale by the Company in order to provide up-to-date information to the clients of the Company when using the Site, as well as to summarize and analyze information about which sections of the Site and products are in greatest demand among clients of the Company;
- processing and storing search queries from users of the Site in order to summarize and create client statistics on the use of sections of the Site.
The company automatically receives some types of information obtained in the process of user interaction with the Site, correspondence by e-mail, etc. We are talking about technologies and services, such as web protocols, cookies, web marks, as well as applications and tools of the specified third sides.
At the same time, web marks, cookies and other monitoring technologies do not make it possible to automatically receive Data. If the user of the Site, at his own discretion, provides his Data, for example, when filling out a feedback form or sending an e-mail, then only then the processes of automatic collection of detailed information are launched for the convenience of using the websites and / or to improve interaction with users.
10.4. Data usage
The Company has the right to use the provided Data in accordance with the stated purposes of their collection with the consent of the Data subject, if such consent is required in accordance with the requirements of the legislation of the Russian Federation in the field of Data.
The obtained Data in a generalized and impersonal form can be used to better understand the needs of buyers of goods and services sold by the Company and to improve the quality of service.
10.5. Data transfer
The Company may entrust the processing of the Data to third parties only with the consent of the Data subject. Also, the Data may be transferred to third parties in the following cases:
a) As a response to legitimate requests from authorized state bodies, in accordance with laws, court decisions, etc.
b) Data cannot be transferred to third parties for marketing, commercial and other similar purposes, except in cases of obtaining the prior consent of the Data subject.
10.6. The site contains links to other web resources, which may contain useful and interesting information for users of the Site. However, this Policy does not apply to such other sites. Users who follow links to other sites are advised to familiarize themselves with the Data processing policies posted on such sites.
10.7. The Site user can revoke his consent to the processing of Data at any time by sending a message by calling the Company's phone number: 88005550486, to the Company's email address: [email protected], through the Company's feedback form located at:, or by sending a written notice to the Company's address: 197342, St. Petersburg, st. Serdobolskaya d.64, building 1, lit.A, office 514. After receiving such a message, the processing of the User's Data will be terminated, and his Data will be deleted, unless the processing can be continued in accordance with the law. Final Provisions This Policy is a local regulation of the Company. This Policy is publicly available. The general availability of this Policy is ensured by its publication on the Company's Website. This Policy may be revised in any of the following cases:
- when changing the legislation of the Russian Federation in the field of processing and protection of personal data;
- in cases of receipt of instructions from the competent state authorities to eliminate inconsistencies affecting the scope of the Policy;
- by decision of the management of the Company;
- when the purposes and terms of Data processing change;
- when changing the organizational structure, structure of information and / or telecommunication systems (or the introduction of new ones);
- when applying new technologies for processing and protecting Data (including transmission, storage);
- when it becomes necessary to change the data processing process related to the activities of the Company. In case of failure to comply with the provisions of this Policy, the Company and its employees are liable in accordance with the current legislation of the Russian Federation. Control over the fulfillment of the requirements of this Policy is carried out by the persons responsible for organizing the processing of the Company's Data, as well as for the security of personal data.