- damage to the bone with a violation of its integrity. With all types of fractures of the upper jaw, swelling of the soft tissues of the perioral zone occurs. Abrasions and lacerations are usually determined on the skin of the face. The height of the face is lengthened, the horizontal parameters are flattened. Localization of bone protrusions, hemorrhages corresponds to the level of damage. The bite is broken. The soft palate shifts downward. The diagnosis of a fracture of the upper jaw is based on the patient's complaints, clinical examination, and CT scan results. Temporary immobilization is carried out prior to the provision of specialized care. The main method of treatment is osteosynthesis with titanium miniplates.

General information
Fracture of the upper jaw is a pathological condition that occurs when the anatomical integrity of the bone is violated. In 1901, the French physician Rene Le Fort proposed the most complete classification of fractures of the upper jaw. Fractures of the upper jaw account for about 4% of the total number of injuries to the maxillofacial region. In the overwhelming majority of cases, men become patients. The most common diagnosis in dentistry is medium fractures of the upper jaw (44%), accompanied by rupture of the mucous membrane and bleeding. Closed fractures are extremely rare. In 15% of cases, not isolated, but combined lesions are observed, in which the violation of integrity is also determined in the surrounding tissues.
Causes
The facial skeleton consists of 3 paired vertical complexes - zygomatic-maxillary, naso-maxillary and pterygo-maxillary and one unpaired median septal-vocal support. Between the vertical lines in the horizontal direction are the alveolar process, the orbit, the superciliary arches, which together strengthen the facial skeleton. As a result of high-energy injuries (hitting the face with a heavy object, falling, in the event of an accident) deflection and collapse of these supporting structures develop, resulting in a fracture of the upper jaw.
The trajectory of movement of the broken off fragments in case of a fracture of the upper jaw depends on the traumatic force, the place of attachment of the masticatory muscles, the area of the fragment. Posteriorly, the damaged fragment is displaced under the influence of the kinetic energy of the impact, downward - as a result of muscle traction. The medial pterygoid muscles contribute to the uneven movement of the fragments in the downward direction, as a result of which the posterior fragments are displaced more than the anterior ones.
Classification
Upper jaw fractures are divided into 3 groups:
- Le Fort 1- upper fracture of the upper jaw. Occurs when an orbital site is injured or when an oblique impact relative to the vertical anatomical structures of the facial skeleton. The damaged maxillary-zygomatic complex is detached from the bones of the skull. Patients have characteristic neurological symptoms.
- Le Fort 2- Medium fracture of the upper jaw. The main reason is a strong direct blow to the area of the nasal bones with closed jaws. Also, type 2 fractures of the upper jaw can occur with reflected damage to the chin, when the traumatic force is transmitted to the upper jaw through the lower teeth. In this case, the separation of the mass, including the maxillary bone and the bones of the nose, occurs.
- Le Fort 3- lower fracture of the upper jaw. It occurs when the upper lip is damaged at the moment when the jaws are open. In this case, the alveolar process loses support and remains open, as a result of which, upon impact, the lower part of the upper jaw is separated from its body. Violation of integrity is also detected in the area of the lower walls of the maxillary sinuses.
Symptoms of fractures of the upper jaw
In patients with type 3 fracture of the upper jaw, swelling of the upper lip, impaired nasal breathing are revealed. The main complaints are reduced to soreness in the area of the injured jaw, an increase in pain syndrome when the teeth are closed. If there is no displacement of the fragment with a fracture of the upper jaw, the fissure-tubercular contact is normal. As a result of the movement of the damaged distal area downward, the patient indicates the presence of a foreign body in the throat. Depending on the trajectory of displacement of the fragment, there may be a violation of the closure of the teeth in the sagittal, transversal or vertical planes.
With a type 2 fracture of the upper jaw, hemorrhage is localized in the tissues around the orbit, resulting in chemosis, exophthalmos. The horizontal parameters of the face are flattened, the vertical ones are lengthened. Soreness increases when the teeth are compressed. With type 2 fracture of the upper jaw, the sense of smell decreases, lacrimation appears. The tongue of the soft palate is deployed downward.
A Le Fort 1 fracture of the upper jaw is combined with damage to the bones of the base of the skull. Patients have severe tissue edema. The conjunctiva, sclera, and tissues of the periorbital area are impregnated with blood. Displacement of the tongue of the soft palate downward causes sore throat, nausea. Dislocation posteriorly of the upper jaw can lead to mechanical asphyxia due to blockage of the airways. If the optic and oculomotor nerves are damaged, vision is impaired, and strabismus may develop.
Diagnostics
An extraoral examination of patients with type 3 upper jaw fracture reveals a violation of the integrity of the zygomatic-alveolar ridges: tissue edema, abrasions, an increase in the vertical parameters of the face. At the border of the transition of the immobile mucous membrane of the alveolar process to the mobile one, as well as on the hard palate, hemorrhages are diagnosed. Displacement of the damaged sections with a fracture of the upper jaw leads to rupture of the mucous membrane. The downward dislocation of the posterior fragment is the cause of the lengthening of the soft palate.
In the course of palpation examination on the alveolar process, irregularities and retractions are determined. When pressing on the hooks of the pterygoid processes, the patient feels pain in the area corresponding to the fracture line of the upper jaw. More often, disocclusion is observed in the anterior region, less often bite pathologies are diagnosed along the transversal and sagittal. Touching the tip of the probe to the mucous membrane of the alveolar process, the patient does not feel, which indicates a loss of pain sensitivity. On CT with a type 3 maxilla fracture, areas of integrity violation in the areas of the pear-shaped aperture and zygomatic alveolar ridges, a decrease in the transparency of the maxillary sinuses are revealed.
In case of type 2 fracture of the upper jaw, the symptom of glasses is positive - the periorbital zone is soaked with blood immediately after damage. Chemosis, exophthalmos, lacrimation are observed. Pain sensitivity of the skin in areas corresponding to the level of damage is reduced. In the anterior region, as a rule, disocclusion. During palpation, the dentist determines the mobility of the maxillary bone at the border with the orbit, in the area of the zygomatic alveolar ridge, as well as in the area of the suture connecting the frontal bone with the upper jaw. The same changes can be diagnosed during an X-ray examination.
With a type 1 fracture of the upper jaw, diplopia, chemosis, exophthalmos, subconjunctival hemorrhages, and eyelid edema are observed. If the patient lies, enophthalmos is detected. In a sitting position, the diplopia increases, when the teeth are closed, it decreases. Palpation with an upper fracture of the upper jaw, it is possible to reveal an unevenness in the areas of the maxillary, as well as the zygomatic-frontal sutures, the zygomatic arch. The load test is positive. On computed tomography, a violation of integrity is found in the area of the root of the nose, the zygomatic arch, the fronto-zygomatic suture, the sphenoid bone. A diagnostic test that determines the presence of rhinorrhea is a sample of a handkerchief. After drying, the structure of the tissue impregnated with liquor remains unchanged. If the scarf has become rigid, then there is no liquorrhea, serous contents are released from the nasal passages.
It is necessary to differentiate a fracture of the upper jaw with other injuries to the bones of the maxillofacial skeleton. All patients should be examined by a maxillofacial surgeon as well as a neurologist. In case of damage to the maxillary sinuses, optic nerve, skull bones, treatment is carried out in conjunction with a neurosurgeon, resuscitation specialist, ophthalmologist, otorhinolaryngologist.
Treatment of fractures of the upper jaw
Treatment of fractures of the upper jaw consists of the stages of reduction, fixation of fragments, immobilization of the bone. When transporting a patient to a specialized institution, bandages are applied to the frontal bone and chin to provide temporary fixation of the maxillofacial complex. Craniofascial attachment in case of a fracture of the upper jaw involves the use of dental splints together with a horseshoe brace, which is installed in the area of the frontal bone.
In the surgical method of treating fractures of the upper jaw, the damaged fragments are repositioned with their subsequent fixation to the healthy bones of the facial skeleton. The most common method of osteosynthesis is the use of wire sutures and titanium miniplates connecting the damaged and immobile bones of the maxillofacial area. In case of fractures of the upper jaw of types 2 and 3, a titanium screw is inserted into the zygomatic bone, since it is this bone that is the nearby support for the damaged fragment.
The access is made along the transitional fold in the projection of the upper jaw fracture. The muco-periosteal flap is peeled off, skeletonizing bone fragments. Titanium screws are threaded into the zygomatic bone and into the alveolar ridge between the large molars at a 90-degree angle to the fracture line. After repositioning the fragments, the screws are interconnected using a titanium wire, the ends of which are twisted. After laying the mucoperiosteal flap, the wound is sutured.
In case of a type 3 fracture of the upper jaw, an incision is made along the line of the outer edge of the orbit. A flap is peeled off in the area of the zygomatic process of the frontal bone, a titanium screw is inserted. The ligature is carried out around the head of the miniplate and under the zygomatic bone, removed in the eve of the oral cavity between the molars, where it is fixed to the head of the second screwed in screw. With timely treatment of a fracture of the upper jaw, the prognosis is favorable. Callus formation occurs within 2 months. Post-traumatic edema resolves within 7 days, subconjunctival hemorrhages persist for several weeks. With late treatment, an incorrect fusion of fragments occurs. In this case, it is necessary to reposition the bone fragments after the renewal of the fracture line of the upper jaw.
Violation of the integrity of the upper jaw requires more efforts than damage to the lower one. The fracture is one of the most dangerous forms lesions with a difficult recovery course. The upper jaw is connected to the facial skeleton and the base of the skull.
The contour of the fracture is difficult to predict. Fragile walls of joints after destruction lead to multiple ruptures of vascular and nerve connections, fragments with cutting edges. High risk of trauma affecting the brain area.
Causes of fractures
Among the injuries of the maxillofacial region, injuries of the upper section occur in 4-5% of cases.
The overwhelming majority of victims are men who have become victims:
- strong blows to the facial area;
- road traffic accidents;
- sports injuries;
- falls face down;
- beatings with brass knuckles;
- combat wounds;
- industrial accidents.
The severity of the fracture is measured by the depth of displacement and downward traction. The maxillary bone is broken out in part along the line of minimum resistance with channels and holes for neurovascular connections.
Views

The initial stage of diagnosing a fracture practically coincides with the generally accepted types:
- open or closed form;
- presence or absence of bias.
Closed fractures, according to statistics, are very rare. The forms of maxillary fractures with rupture of soft tissues, bleeding prevail. Injuries with concomitant damage to other organs are characteristic.
The severity is characterized by faults of the following types:
- Upper. The contour of the fracture is along the line of the floor of the maxillary sinus. The most dangerous break, as it differs in the mobility of bones, structures of the nose, cheekbones. It is accompanied by loss of consciousness, brain disorders.
- Average. Fracture line between nose and eye socket. The mobility of fragments of the jaw and nose is noted.
- Lower. Fracture from the base of the nose to the cheekbones. The upper jaw and palate are mobile.
Injuries are characterized by common symptoms and private, according to the classification proposed by the surgeon Rene Le Fort. He gave a description of the signs, the development of the lesion, ways of providing assistance.
Le Fora's classification and characteristic symptoms
The most complete detailing proposed by the French physician is based on the analysis of faults along lines of weak resistance in the structure of bone joints. Each type of fracture is characterized by specific symptoms, in addition to general manifestations.
The symptoms of maxillary fractures are as follows:
- displacement of the dentition, change in bite;
- face contour transformations;
- acute pain when moving the mouth;
- bleeding from the ears, nose, mouth;
- swelling of the face and bruises;
- unnatural movement of the jaw.
In some cases, the signs are not pronounced, therefore, the visit to the doctor is delayed. Loss of time significantly exacerbates the dysfunction and complicates the provision of care.
Symptoms
Upper Le Fort 1... Damage to the maxillary zygomatic complex is associated with separation from the bones of the skull, almost the contour of the fracture reflects the puncturing of the facial region from the skull. There is a fracture of the ethmoid bone, the nasal septum. The outflow of cerebrospinal fluid into the pharynx, nose, ears, the main neurological symptoms indicate an injury to the base of the skull. Damage to the optic nerve leads to bifurcation or loss of visual fields, decreased acuity, impaired ocular motility, sensation, loss of sensitivity in the upper eyelid region.
The displacement of the palate gives the feeling of a foreign object in the throat, nausea. The outline of the shape of the face changes towards an increase in height. The palpebral fissures widen, the eyeballs descend.
X-ray images show fractures of the zygomatic arches, nose. Side views show the fracture lines of the sphenoid bones.

Middle Le Fort 2... The fracture line almost coincides with the boundaries of the maxillary bone. The slit runs in the medial or lateral direction. Damage to the lower part of the eye sockets is recorded. Suborbital fracture is accompanied by profuse bleeding from the nose and mouth. The main problems are manifested in double vision (diplopia), difficulty swallowing, vomiting, and difficulty swallowing.
In connection with pinching or detachment of the olfactory filaments, the corresponding function is lost. The appearance of blood from the lacrimal canal is likely due to its deformation. There is a loss of sensitivity (stiffness) of the facial areas: nose, lower eyelids, front teeth, upper lip.
The face is distorted by large swelling and tissue hemorrhage. Hematomas, air imphysema interfere with the examination of the eyes. In the horizontal position, the face has a flattened appearance, and in the vertical position, the shape is elongated downward.

Swelling of the walls of the pharynx, drooping of the palate, a low tone with percussion of the teeth are recorded. The roentgenogram reflects the contour of bone fracture at the base of the nose, the lower edges of the orbits, and the presence of blood in the maxillary cavities.
Lower Le Fort 3. The fracture is formed when the jaws are open. The alveolar process loses support, the impact force separates the lower part of the upper jaw. The nasal fundus with the maxillary cavity breaks off. Accordingly, the sensitivity and functionality of structures with torn nerve trunks is impaired.
Patient complaints reflect loss of sensitivity of the palate and teeth, difficult nasal breathing, malocclusion, inability to bite off food, and gagging.
During the examination, there is an elongation of the face in the lower part, a drooping of the palate, and blood effusion into the jaw folds. On palpation, crepitus is diagnosed in the area of the nose, eye sockets.
Radiography reflects deformation of the pear-shaped holes, fractures of the zygomatic alveolar ridges, hemorrhages in the maxillary cavity.
Diagnostics

Patients are examined by specialists in maxillofacial surgery and neuropathologists. Complex injuries additionally require the participation of neurosurgeons, ophthalmologists, resuscitators, and otorhinolaryngologists.
Differential diagnosis is carried out on the basis of a clinical examination and radiographs. But ordinary snapshots are not enough. The complex structure of the facial region, layering of bones impede obtaining complete information. An overview projection is used to reflect the skull from different sides. But the debris trapped inside cannot always be seen. The axial projection method assists in the detection of fragments.
MRI examination, CT scan assist in the accurate diagnosis of damage to the facial, intracranial bones. Clinical observations reflect typical fractures systematized in the history of surgery. Of particular difficulty are gunshot wounds.
Massive edema interferes with the initial examination. Temporary immobilization is carried out prior to the provision of specialized assistance measures. Thanks to accurate diagnosis, after 8-10 days, they begin to simultaneously compare the bones of the skull and the facial region.
The combination of injuries with the inclusion of a fracture of the upper jaw is manifested by the syndrome of mutual burden. Patients have an increased risk of developing septic complications in the lesions, metastasis of the infection.
First aid

The actions of people who witness severe trauma can play a decisive role in the life of the victim, especially with bleeding or asphyxiation.
It is necessary to distinguish the nature of assistance, on which the prognosis for survival, cure depends:
- mutual assistance at the scene;
- assistance of the medical personnel on duty who arrived on call;
- first aid by non-medical professionals within 4 hours of injury.
The arrived first aid personnel evacuate the patient, monitor the patient's condition in general.
There are cases of discrepancy between the appearance of a person and the severity of damage. He can get to the emergency room on his own, but the manifestation of symptoms will increase, the deterioration of the condition will progress rapidly.
The nursing staff examines the victim and performs primary therapeutic and prophylactic measures to prevent wound infection, further bleeding, and asphyxiation. Anti-shock measures include pain relief, immobilization.
At the scene, it is important to prevent mechanical asphyxia as a result of tongue retraction, teeth debris entering the respiratory tract, and severe bleeding. To do this, the position of the victim should be on the side with the head turned towards the wound or down. An aseptic napkin should be put in place of the injury, lightly pressed to stop bleeding.
The continuity of actions of the medical staff from first aid at the scene of the incident to medical measures in the hospital is very important, it contributes to a favorable outcome and a reduction in the recovery period of the victim.
Treatment

Timely treatment without complications gives a favorable prognosis. Callus is formed in 2 months. Swelling of soft tissues resolves in 7-10 days. Subconjunctival hemorrhages persist for several weeks.
The solution to the problem of healing the upper jaw consists of successive stages:
- Reposition of fragments.
- Fixing the parts in the correct position.
- Strengthening tissue regeneration in the damaged area.
- Prevention of complications.
The specialized help received in a timely manner creates a favorable prognosis for the healing of soft tissues and bone regeneration.
The most famous by means of surgical osteosynthesis are aimed at eliminating bone mobility until complete fusion. Wire sutures, titanium mini-plates are used to connect the bones of the maxillofacial region. In some cases, the zygomatic bone and the alveolar process serve as a support for fixing the titanium screw and connecting the damaged fragments.
Complications

Delayed treatment creates a high risk of abnormal fusion of the fragments, which leads to the need to renew the fracture line of the bone. Postoperative changes in the facial skeleton affect the emotional state of the victim. Additional correction is carried out using modern methods of plastic surgery.
Complications often occur in elderly people: the formation of false joints, the occurrence of osteomyelitis. Special orthopedic constructions are used depending on the type of anatomical disorder.
The treatment of children has its own characteristics. The strength of the jaw is reduced by the absence of root processes of the permanent teeth. A complication is damage to their primordia. Subsequently, there is an incorrect bite, an incorrect position of the teeth.
Power features

The patient is forced to significantly change the diet during the period of treatment and recovery. The immobility of the jaw prevents a full intake of food. Basic nutritional requirements:
- creamy consistency;
- lack of solid and large fragments.
Main dishes: boiled cereals, soups, broths, dairy products, mashed fruits and vegetables. Subsequently, the transition to the usual diet should be gradual.
Consequences

In the case of incomplete treatment, the occurrence of complications during the recovery period, the following formations occur:
- interdental gaps;
- displacement of the dentition;
- development of sinusitis;
- abnormal bite;
- distortion of the oval of the face.
As a result of trauma, mental and neurological disorders, pathologies of individual systems sometimes persist. It is important to prevent the onset of complications in a timely manner in consultation with specialist doctors.
A trauma to the upper jaw affects the deformity of the entire face if specialized treatment is ignored. Qualified help and the patient's desire to restore the correct appearance are important conditions for a successful recovery.
1. Anatomical structure of the upper jaw and borderline bones.
The anatomical features of the upper jaw affect the clinical signs of damage and determine the nature of the fracture.
So, the upper jaw, being a paired bone and located in the center of the face, is connected with other bones of the facial and cerebral skull: zygomatic, frontal, nose bones, ethmoid, wedge-shaped, lacrimal.
There are four surfaces of the body of the upper jaw: anterior, infratemporal, orbital, nasal (Fig. 21).
Front surface(facies anterior) bounded from above by the inferior orbital edge, laterally by the zygomatic ridge and zygomatic process, below by the alveolar ridge and medially by the nasal notch. Under the inferior orbital edge is the infraorbital foramen (for. Infraorbitale), through which the terminal branch of the nerve and vessels of the same name emerges.
Subtemporal surface(facies infratemporalis), represented by the tubercle of the upper jaw. The oblique head of the lateral pterygoid muscle is attached to it. In the tubercle of the upper jaw there are 3 - 4 holes through which the posterior upper alveolar branches enter the thickness of the bone tissue, which take part in the formation of the posterior part of the upper dental plexus.
Rice. 21. Schematic representation of the upper jaw: 1-lower orbital edge; 2-zygomatic alveolar ridge; 3-alveolar process; 4-nasal cavity; 5-infraorbital foramen; 6-tubercle of the upper jaw; 7- nasal spine; 8-zygomatic bone.
Orbital surface(facies orbitalis) takes part in the formation of the lower wall of the orbit and forms the lower orbital edge. In the posterior part, together with the orbital edge of the large wings of the sphenoid bone, it limits the inferior orbital fissure (fissura orbitalis inferior). Through it, the infraorbital nerve (n. Infraorbitalis), a branch of the maxillary nerve, enters the orbit. The latter passes in the infraorbital sulcus and in the infraorbital canal, which are located on the orbital surface of the upper jaw body. The lower wall of the canal is pierced with small anterior and middle upper alveolar openings (foramina alveolaria superiora anteriora et media). They lead to small bony canals that extend to the roots of the incisors, canines and small molars. Vessels and nerves pass through them to these teeth. The medial edge of the orbital surface is bordered by the lacrimal bone, the orbital plate of the ethmoid bone and the orbital process of the palatine bone. Sometimes it forms cells that are directly adjacent to the cells of the ethmoid labyrinth.
Nasal surface(facies nasalis) is connected to the perpendicular plate of the palatine bone, with the inferior nasal concha and the hook-shaped process of the ethmoid bone. Between the lower and middle shells is the opening of the maxillary sinus - the maxillary cleft (hiatus maxillaris). Anterior to the cleft is the nasolacrimal canal (canalis nosolacrimalis), which opens into the nasal cavity. The lacrimal bone and the lacrimal process of the inferior turbinate take part in its formation. Behind the maxillary cleft, there is a large palatine canal formed by the palatine bone and the pterygoid process of the sphenoid bone.
In the area of the upper jaw, four processes are distinguished: frontal, alveolar, palatine and zygomatic.
Frontal process(processus frontalis) with the inner edge connected to the nasal bone, the upper one with the nasal part of the frontal bone, the posterior one with the lacrimal bone. Consists mainly of a compact substance. It is able to withstand a compressive load from the bottom up to 470 - 500 kg, which is much more than the pressure force developed by the masticatory muscles.
Zygomatic process(processus zyqomaticus) connects to the zygomatic bone. Downward, between it and the hole of the first molar, is the zygomatic-alveolar ridge. The zygomatic process consists mainly of a compact substance.
Palatine process(processus palatinus) is horizontal. Anteriorly and outwardly, it passes into the alveolar process, the inner surface is connected to the palatine process opposite side, behind - with a horizontal plate of the palatine bone. The nasal crest (crista nasalis) is located along the inner edge of the process, which connects to the cartilaginous part of the nasal septum. The medial edge of the process from the palatal surface is thickened. On the upper surface of the palatine process, on the side of the nasal crest, there is an incisal opening, which leads to the incisal canal (canalis incisivus). In the anterior 2/3, the process consists of compact and spongy substances. In the posterior third, there is no spongy substance, and in this section it is much thinner than in the anterior one. The palatine process is marked by increased strength.
The alveolar process (processus alveolaris) consists of the outer and inner plates of a compact substance, between which there is a spongy substance. The outer plate is thinner than the inner one, at the level of the premolars - thicker than that of the anterior group of teeth.
An airway is located in the body of the upper jaw. maxillary sinus, the walls of which are represented by thin bone plates of a compact substance. The maxillary sinus is the largest of the paranasal sinuses. It can spread to the alveolar, zygomatic, frontal and palatal processes. It distinguishes between the upper, lower, medial, anterolateral and posterolateral walls, covered with a mucous membrane.
Top wall, separating the maxillary sinus from the orbit, it is represented mainly by a compact substance with a thickness of 0.7 to 1.2 mm. It thickens at the inferior orbital margin and zygomatic process.
Bottom wall the sinus has the shape of a groove where the medial, anterolateral and posterolateral walls join. The bottom of the wall is either even or represented by tubercle protrusions above the roots of the teeth. The thickness of the compact plate separating the bottom of the maxillary sinus from the holes of the first and second large molars may be insignificant and not exceed 0.3 mm.
Medial wall consists only of a compact substance and borders on the nasal cavity. It has a great thickness (about 3 mm) in the region of the anterior-inferior corner, the smallest (1.7 - 2.2) - in the middle of its lower edge. Behind it passes into the posterolateral wall. At the place of this transition, it is very thin. In front, the medial wall passes into the anterolateral, where it thickens. In the upper-posterior part of the wall, there is a maxillary cleft (hiatus maxillaris), which connects the sinus with the middle nasal passage.
Anterolateral wall the sinus in the area of the canine fossa consists of a compact substance and in this place is the thinnest (0.2 - 0.25 mm). It thickens with distance from the fossa, reaching a greater thickness (up to 6.4 mm) at the lower edge of the orbit. The alveolar, zygomatic, frontal processes of the inferolateral edge of the orbit have a spongy substance. In the anterolateral wall, there are several alveolar bone tubules, where nerve trunks and vessels pass to the frontal teeth and premolars.
Posterolateral the wall is represented by a compact plate, which bifurcates at the transition to the zygomatic and alveolar processes. There is a spongy substance here. In the upper section, it is thinner than near the alveolar process. In the thickness of the nerve trunks are located, going to the large molars.
Thus, the upper jaw takes part in the formation of the orbit, nasal cavity and mouth. She is directly related with the zygomatic, palatine, frontal, nasal, lacrimal, ethmoid, sphenoid bones.
The frontal, ethmoid, sphenoid and temporal bones form the anterior and middle cranial fossa.
The walls of the maxillary sinus are represented by thin bony plates. Nevertheless, the upper jaw is able to withstand significant mechanical stress. This is due to the fact that the trabeculae of the spongy substance have a predominantly vertical type of structure, and the compact substance is thickened in certain areas, or buttresses.
There are 4 buttresses:
1. Frontal-nasal. Corresponds to the anterior group of teeth. It rests on the somewhat thickened walls of the canine alveoli, located along the edge of the nasal opening and the frontal process of the upper jaw to the nasal process of the frontal bone.
2. Sculoalveolar. It starts from the second premolar, first and second molars. It continues along the zygomatic alveolar ridge towards the body of the zygomatic bone and the zygomatic process of the frontal bone. Through the zygomatic arch, pressure is transmitted to the temporal bone. It is the most powerful buttress, taking the pressure from the above teeth.
3. Pterygoid-jaw. Formed by the pterygoid process of the sphenoid bone and the tubercle of the upper jaw. These anatomical structures are fused together and form a fairly strong bone structure. Resists the chewing pressure developed by the large molars, mainly the second and third molars.
4. Palatine. Formed by the palatine process of the upper jaw and represented by two longitudinal grooves running along the bottom of the nose. In the area of the nasal notch, it connects with the frontal-nasal cotrofors, which, in turn, is associated with the zygomatic alveolar in the region of the upper and lower edges of the orbit. The alveolar process combines the zygomatic alveolar, pterygopalatine and palatal buttresses.
The above anatomical features determine the resistance of the upper jaw to chewing pressure and its ability to withstand significant mechanical stress.
2. Clinical picture and diagnosis of fractures of the upper jaw.
Areas of increased strength of the upper jaw depend on the structure of bone tissue associated with its formation in phylogenesis. Strong places correspond to ossification points, weak ones - to intermediate lines. In a non-firearm fracture of the upper jaw, the fracture lines run along the sutures connecting it to the other bones of the facial skeleton, as well as to the bones that form the base of the skull. It is along them that the zone of reduced bone strength is predominantly located. This can explain why most often the fracture line does not pass strictly within the anatomical boundaries of the upper jaw, but extends to adjacent bones associated with it. Therefore, in the clinic, one has to deal not so much with a fracture of the upper jaw itself, as with breaking it out with areas of other bones of the face and the base of the skull. This is what determines the variety of clinical manifestations, the severity of the course and various outcomes of injuries of the upper jaw.
In clinical practice, most doctors use the classification proposed by Le Fort in 1901, which experimentally identified and described various types of fractures of the upper jaw. In accordance with the order of their description, the author highlighted: upper(Le Fort I), average(Le Fort II), lower(Le Fort III) types of fractures. According to this classification, fractures of the upper jaw are bilateral, and their lines are symmetrical. Meanwhile, clinical experience and literature data indicate that there are often exceptions to this rule.
Upper jaw fractures account for 2 to 5% of facial fractures. Their cause is a serious mechanical injury: a road traffic accident, a victim's fall facedown from a height, a heavy object falling on his face (ground, fragments of reinforcement, a sports equipment, etc.), a kick in the face, etc. These fractures, as a rule, accompanied by traumatic brain injury. The broken off upper jaw can be displaced posteriorly - in the direction of the applied force; down - due to the own severity of the fragment, as well as due to the traction of the medial pterygoid and the masseter muscle itself (with a fracture of types I and II).
At the same time, it shifts downward unevenly: the posterior sections of the upper jaw are displaced more than the anterior ones, which is associated with the traction of the medial pterygoid muscle (see the function of the masticatory muscles of the posterior group). In the event of exposure to a traumatic force at an angle to the frontal plane, the fragment can be displaced in the direction opposite to the applied force.
2.1. Clinical picture and diagnosis of fractures of the upper jaw according to the Le Fort I type (upper type).
The fracture gap passes in the area of junction of the frontal process of the upper jaw with the nasal part of the frontal bone in the area of its ethmoid notch.
The anterior edge of the latter connects to the nasal bones, and the posterior edge to the anterior edge of the perforated plate of the ethmoid bone, which participates in the formation of the base of the skull in the region of its anterior fossa. The posterior sections of the nasal part of the frontal bone contain cells that are in contact with the ethmoid bone and form the roof of its cells. Further, the fracture line extends along the inner wall of the orbit to the junction of the upper orbital and lower orbital fissures, then along the outer wall of the orbit, directed upward and anteriorly to its upper outer corner. Here it runs along the frontal-zygomatic suture, then - posteriorly and downward along the large wing of the sphenoid bone to the lower surface of the body and the upper part of its pterygoid process. The zygomatic process also breaks temporal bone and the septum of the nose (Fig. 22).
 Rice. 22. Scheme of the fracture of the upper jaw according to the Le Fort I. Front view.
Rice. 22. Scheme of the fracture of the upper jaw according to the Le Fort I. Front view.
Thus, in a Le Fort I fracture, the upper jaw is separated, along with other facial bones, from the bones of the cerebral skull.
In the anatomical boundaries of the upper jaw, the fracture occurs only in the region of the frontal process and the posterior parts of its orbital surface, and mainly along the adjacent bones. The broken bone conglomerate, in addition to the upper jaw, includes a paper plate of the ethmoid bone, the lacrimal bone, part of the frontal, zygomatic and sphenoid bones. It is known that the orbital surface of the frontal bone, ethmoid bone and the body of the sphenoid bone form anterior cranial fossa, and the body and large wing of the sphenoid bone take part in the formation of the middle cranial fossa.
Consequently, a Le Fort I fracture of the upper jaw is inevitably accompanied by a fracture of the base of the skull.
This type of fracture can be attributed to a fracture of only the upper jaw conditionally and the terms existing in the literature "Craniofacial separation", "subbasal fracture" more accurately reflect its essence: as a fracture of the bones of the middle zone of the face.
A Le Fort I fracture is the most severe: signs of a fracture of the base of the skull and brain damage of varying severity prevail. Nevertheless, it is possible to identify clinical signs that are characteristic of this particular type of fracture, when they are not masked by symptoms of brain damage.
While maintaining consciousness and satisfactory orientation, the patient complains of double vision with an upright body position, decreased visual acuity, painful and difficult swallowing and mouth opening, improper closing of teeth, foreign body sensation in the throat, retching, choking and nausea. The latter signs are not associated with brain injury, but arise as a result of mechanical irritation of the reflexogenic zone of the posterior pharyngeal wall or the root of the tongue with a small tongue that has shifted posteriorly and downward along with the hard and soft palate.
It is noted pronounced edema in the eyelids, root of the nose, infraorbital, buccal and temporal regions. The patient's face becomes moon-shaped. In the area of the zygomatic arches, sinking of tissues. Well defined hemorrhage in the upper and lower eyelids, as well as other tissues of the periorbital zone, the conjunctiva, which is called "Glasses symptom".
Sometimes the swelling of the conjunctiva is so significant that it bulges out between the closed eyelids. In the horizontal position of the patient in bed, his face is flattened, enophthalmos may be noted. When the patient moves to a sitting position (vertical), the face lengthens, the eyeballs move downward, and the palpebral fissure expands. Subjectively, this is accompanied by increased diplopia. Sometimes the patient, trying to eliminate diplopia, closes one eye with his palm or brings his finger under the eyeball, lifting it.
The opening of the mouth is limited. If you ask the patient to close his teeth tightly, it can be noted that the eyeballs move upward, and the palpebral fissure narrows, subjectively - double vision decreases. The return of the patient to a horizontal position in bed is accompanied by a flattening of the face and a change in the relationship between the teeth of the upper and lower jaws, a decrease in diplopia. Sometimes palpation can determine bony protrusion between the nasal part of the frontal bone and the frontal process of the upper jaw, as well as in the area of the zygomatic-frontal suture (upper-outer part of the orbit) and the zygomatic arch.
Occasionally, in the area of the root of the nose, crepitus, caused by air emphysema.
In case of damage to the orbital nerve (n. Ophthalmicus), pain sensitivity of the skin in the forehead, upper eyelid, inner and outer corners of the palpebral fissure decreases or disappears.
Opening the mouth is accompanied by soreness in the upper jaw. With the maximum opening of the mouth, the distance between the upper and lower incisors is less than normal, due to the downward displacement of the upper jaw. An open bite is determined. However, other options for the relationship of the dentition are also possible, which depends on the degree of displacement of the broken off fragment to the side, back, down and on the patient's bite.
When the teeth of the upper jaw are percussed, a dull (low) sound is noted.
The soft palate shifts posteriorly and downward. Its tongue touches the root of the tongue and the back of the pharynx. When pressing on the hooks of the pterygoid processes of the sphenoid bone, hard palate or the last molars, pain is noted along the course of the alleged fracture gap (positive symptom of exercise).
Not strong and prolonged (1 minute) pressure on the hard palate upwards leads to a shortening of the middle zone of the face, narrowing of the eye slits and wrinkling of the skin at the root of the nose.
When grasping the alveolar process in the frontal area with the fingers of the right hand and extremely careful displacement of the bone fragment in the anteroposterior direction, it is possible with the second finger of the left hand, placed in the places of the identified bone steps, to determine synchronous mobility in the frontal-nasal and frontal-zygomatic regions and along the length of the zygomatic arcs. If such steps were not installed earlier, then when the upper jaw is displaced, it is necessary to carefully examine the glabella, all the edges of the orbit and the zygomatic arch with the second finger of the left hand.
The detection of pathological mobility of the upper jaw is direct evidence of its fracture.
Sometimes an additional fracture occurs in the sagittal plane, that is, the upper jaw is separated into two halves. The fracture gap never runs along the middle suture, but is parallel to it. In such patients, either hemorrhage in the hard palate along the midline and a bone step can be found,
either a laceration of the mucous membrane of the hard palate and a small gap between the fragments lateral to the midline, leading to the nose, or a wide wound resembling a congenital cleft of the hard palate, through which the nasal cavity is visible.
With a fracture of the upper jaw in the upper type, the optic nerve is quite often damaged, which passes in the optic canal located between the body and the small wings of the sphenoid bone. This is manifested by a decrease in visual acuity, sometimes - a loss of visual fields with damage to a part of the optic nerve fibers. The oculomotor (III), block (IV), abducens (VI) and orbital nerves (branch trigeminal nerve). These nerves can also be damaged. In this regard, the patient can only partially open the eye or not open it at all. Perhaps divergent strabismus (damage to the trunk of the III pair). If the movement of the eyeball is limited downward and outward, diplopia when looking under the feet, one should suspect the defeat of the IV pair. Converging strabismus and double vision in the horizontal plane are characteristic of the defeat of the VI pair. Violation of pain sensitivity of the skin in the upper eyelid, outer and inner corner of the palpebral fissure, forehead skin can be with damage to the infraorbital nerve.
When examining patients with suspected fractures of the upper jaw of the Le Fort I type, the participation of a neurologist and neurosurgeon is necessary.
IN clinical practice there are observations when the upper jaw breaks out as a single block with the frontal bone (Billet-Vignell, MB Shvyrkov). In this case, the fracture line begins not at the junction of the frontal process of the upper jaw with the nasal part of the frontal bone, but at the junction of the frontal bone with the parietal, i.e. in the area of the frontal-parietal suture. Then it goes down to the scales of the temporal bone or along the large wing of the sphenoid bone and, passing behind the pterygoid processes of this bone and the lacerated opening, ends at the junction of the sphenoid bone with the occipital. The zygomatic arches must break. This fracture is usually bilateral and the fracture line runs almost symmetrically. When examining the patient, there is also a large swelling of the face. When swinging the upper jaw behind the alveolar process, it is not possible to detect pathological mobility in all typical places. It is found in the region of the frontal-parietal suture and zygomatic arch. A bone step is also found there. There is no large downward displacement of the upper jaw, and the malocclusion is insignificant.
On the radiograph of the facial bones in frontal projection in patients with fractures of the upper jaw of the Le Fort I type, it is possible to establish a violation of the integrity of the bone tissue in the area of the root of the nose, zygomatic arch, greater wing of the sphenoid bone and the frontal-zygomatic joint, as well as a decrease in the transparency of the maxillary and sphenoid sinuses ... On the lateral radiograph, there may be signs of a fracture of the body of the sphenoid bone. In some patients, pneumocephalus is noted - the accumulation of air in the anterior cranial fossa.
2.2. Clinical picture and diagnosis of fractures of the upper jaw according to the Le Fort II type (medium type).
With this injury, the fracture gap passes at the junction of the frontal process of the upper jaw with the nasal part of the frontal bone in the region of its lattice notch, along the inner wall of the orbit to the inferior orbital fissure. Then it spreads anteriorly along the lower wall of the orbit to the lower orbital edge. The fracture gap crosses it along or near the zygomatic-maxillary suture. Then it goes down and posteriorly along the front surface of the upper jaw, crosses the zygomatic alveolar ridge, passes along its infratemporal surface and spreads to the pterygoid process of the sphenoid bone (sometimes on the border of its upper and middle third). The nasal septum breaks (Fig. 23). Sometimes the fracture line passes through the infraorbital canal and through the infraorbital foramen, which is accompanied by damage to the infraorbital nerve.
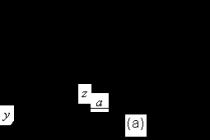
 Rice. 23. Scheme of a fracture of the upper jaw according to the Le Fort II type (a - front view, b - side view).
Rice. 23. Scheme of a fracture of the upper jaw according to the Le Fort II type (a - front view, b - side view).
If the fracture gap at the infraorbital margin is significantly displaced outward and intersects the zygomatic bone, damage to the zygomatic nerve is possible. With this type of fracture, the broken bone conglomerate includes the entire upper jaw with the bones of the nose, the bones that take part in the formation of the base of the skull (frontal, ethmoid, the body of the sphenoid bone), as well as the lacrimal, part of the orbital surface of the zygomatic and palatine bones. Therefore, we can talk about a fracture of the upper jaw together with other bones located next to it.
Terms existing in the literature "Maxillofacial separation" and "Suborbital fracture" most reliably reflect the essence of the fracture of the upper jaw of this type.
In addition to the typical location of the Le Fort II fracture lines, a fracture in the sagittal plane is possible, i.e. passing through the hard palate. It is known that the upper jaws grow together in embryonic period and only palatine processes. Such a fracture is not so much dangerous for the patient as it significantly complicates the fixation of the jaw fragments. Its clinical manifestation is described above.
With a fracture of the Le Fort II type, the probability of a fracture of the base of the skull and damage to the brain is high, this largely depends on the direction of the fracture gap and its location in the area of the bones that form the base of the skull.
The frequency of damage to the ethmoid bone is due not only to the fact that it takes part in the formation of the medial wall of the orbit, but also because the ethmoid notch of the frontal bone, in the zone of which the fracture line passes, is connected with its posterior edge to the perforated plate of this bone.
With a fracture of the Le Fort II type, there may be complaints of pain in the upper jaw, aggravated by closing the teeth and chewing food; sensation of a foreign body in the throat, retching; difficulty breathing not only with the nose, but also with the mouth; sometimes double vision; numbness of the skin in the infraorbital region and upper lip, lower eyelid, wing and cutaneous part of the nasal septum; numbness of the incisors, canines, premolars and the mucous membrane of the alveolar process from the vestibular side within these teeth; sometimes - a decrease or loss of smell in case of rupture or infringement of the olfactory filaments (f. olfactoria) passing through the holes of the perforated plate of the ethmoid bone.
In case of damage (flattening) of the nasolacrimal canal, complaints of lacrimation are possible, which is confirmed by an objective study.
The configuration of the face is changed due to severe post-traumatic edema, sometimes subcutaneous emphysema and hemorrhage in soft tissue infraorbital and zygomatic regions. Localization of hemorrhage in the orbital zone is characteristic.
The soaking of soft tissues with blood is more pronounced in the area of the root of the nose, upper and lower eyelids, conjunctiva and sclera of the eyeball. It is less intense or may not be determined at all, respectively, in the upper-outer quadrant of the orbit, if the hematoma is caused only by bone lesions. However, contusion of the soft tissues of the periorbital zone at the time of injury can determine the uniformity of the location of the hemorrhage zone around the orbit. The hematoma can spread to the supraorbital and infraorbital regions.
Hemorrhage in the tissues of the eyelids and their edema are sometimes so pronounced that it is difficult to examine the eyeball. The saturation of the conjunctiva with blood is so significant that chemosis is expressed, the conjunctiva bulges out between the closed eyelids. With hemorrhage into the retrobulbar tissue, exophthalmos can be determined.
In the horizontal position, the patient's face is flattened due to the posterior displacement of the fragment and the pronounced contouring of the zygomatic bones. In the vertical position, the patient's face is somewhat lengthened due to the displacement of the upper jaw downward, in the horizontal position it is flattened due to the posterior displacement of the fragment.
On palpation of the soft tissues of the infraorbital region and the root of the nose, crepitus is sometimes felt - a sign of subcutaneous emphysema. The latter occurs as a result of exfoliation of the mucous membrane of the maxillary sinus when the fragment of the upper jaw is displaced and a kind of valve is formed. This is accompanied by the creation of negative pressure. When the mucous membrane ruptures, atmospheric air rushes into the zone of reduced pressure and penetrates into the subcutaneous fat.
Pain sensitivity is reduced or absent in the innervation zone of the lesser crow's feet.
On the lower edge of the orbit, a bony protrusion - "step" is clearly palpated. In the area of the root of the nose, it is much more difficult to determine it due to the pronounced edema of the tissues and their sharp soreness. More often, there is a lack of a bone base under the finger in case of displacement of the fragment, occasionally - crepitus due to air emphysema. If you place the index finger of the left hand on the lower edge of the orbit in the projection of the bony protrusion, the big one - on the area of the root of the nose, and with the right hand slightly displace (no more than 2 - 3 mm) the upper jaw in the anteroposterior direction, one can determine the synchronous »Bone fragment under the fingers of the left hand at the same time in both places. In this case, the skin above the root of the nose will fold or change in color due to its uneven tension when the fragment is displaced. Palpation with three fingers of the left hand (1, 2 and 3) of the root of the nose, the infraorbital margin on the left and on the right allows one to verify the synchronous displacement of the fragment at three points.
In case of damage to the nasolacrimal canal, in addition to lacrimation, blood may appear from the lacrimal openings.
Opening the mouth is painful, sometimes limited. The distance between the central incisors with the maximum opening of the mouth is reduced, which can be with a significant downward displacement of the upper jaw.
The bite is broken. More often only molars are in contact (open bite). However, it can be direct, progenic, cross, which depends on the initial ratio of the dentition, the severity and nature of the displacement of the fractured fragment.
When the teeth of the upper jaw are percussed, the percussion sound is low (dull). There is a hemorrhage in the tissue of the upper vestibule of the mouth, respectively, large and partially small molars.
The bony protrusion is palpated in the area of the anterior wall of the upper jaw, the zygomatic alveolar ridge and the region of the tubercle of the upper jaw.
Pain sensitivity of the gingival mucosa is reduced or absent within the incisors, canines and premolars.
The soft palate is displaced posteriorly. The small tongue touches the back of the throat or the root of the tongue. In the upper part of the pterygoid-mandibular fold, the anterior palatine arch and the soft palate, there may be hemorrhage due to its soaking with blood descending from the fracture site in the region of the upper jaw tubercle and the pterygoid process of the sphenoid bone.
In the case of the formation of a hematoma in the periopharyngeal space, the lateral pharyngeal wall protrudes.
The pain symptom of the load is positive: when pressing on the hooks of the pterygoid processes of the sphenoid bone or the upper molars, pain occurs along the fracture line. When determining the pain symptom of a load in the vertical position of the patient, bone fragments are simultaneously displaced upward, respectively, of the frontal process of the upper jaw, the lower edge of the orbit and the zygomatic alveolar ridge, which is determined by palpation. In addition, a fold of skin appears at the root of the nose.
On the radiograph of the facial bones in the naso-chin and lateral projections, it is possible to note a discontinuity of the bone in the area of the root of the nose, the lower edge and the bottom of the orbit, the zygomatic alveolar ridge, and a decrease in the transparency of the maxillary sinuses.
2.3. Clinical picture and diagnosis of fractures of the upper jaw according to the Le Fort III type (lower type).
The fracture gap passes through the edge of the pear-shaped opening posteriorly along the anterior surface of the upper jaw slightly above the bottom of the maxillary sinus. Crosses the zygomatic alveolar ridge, goes along the tubercle of the upper jaw and extends to the lower third of the pterygoid process of the sphenoid bone (Fig. 24). Sometimes the fracture gap ends in the area of the tubercle. In this case, pressure on the pterygoid hook is not painful and may complicate diagnosis. Therefore, more informative information is given by pressure on the hard palate or molars. Very rarely, the fracture line ends at the third molar and does not pass to the pterygoid process.
With a fracture of the lower type, the nasal septum breaks in the horizontal plane, the bottom of the nose and maxillary sinus breaks off. The nerve trunks are torn completely or partially, passing in the bony tubules of the walls of the upper jaw and taking part in the formation of the upper dental plexus or extending from it, which manifests itself in the clinical signs of this type of fracture by a violation of pain sensitivity in the zone of tissues innervated by them. Sometimes there may be a fracture of one upper jaw, then the fracture line must pass through the hard palate in the sagittal plane.
With the lower type of fracture, patients may complain of diffuse pain in the upper jaw, aggravated by closing the teeth or trying to chew food; the inability to bite off food with the front teeth; numbness of all teeth and
 Rice. 24. Scheme of the fracture of the upper jaw according to the Le Fort III type (a - front view, b - side view).
Rice. 24. Scheme of the fracture of the upper jaw according to the Le Fort III type (a - front view, b - side view).
the mucous membrane of the gums, often - the mucous membrane of the hard and soft palate (if the nerves passing in the pterygopalatine canal are injured); on improper closing of teeth; Difficulty nasal and oral breathing; sensation of a foreign body in the pharynx, choking, occasionally - periodic urge to vomit (due to the posterior displacement of the soft palate and irritation of the mucous membrane of the posterior pharyngeal wall with a small tongue, violation of the innervation of the soft palate).
The configuration of the face is changed due to post-traumatic edema of the soft tissues of the lower third of the face (upper lip, buccal, zygomatic regions), hemorrhages in the tissues of the oral region, and sometimes subcutaneous emphysema. The nasolabial folds are smoothed. On the skin of the face there may be abrasions, bruises, lacerations and bruised wounds. In the case of a significant downward displacement of the fragment with an upright position of the patient, the lower part of the face is lengthened. Sometimes it is possible to note the displacement of the skin part of the nasal septum from a horizontal position to an oblique position due to the displacement of soft tissues along with the broken upper jaw downward. However, it is rather difficult to establish this clinical sign due to the pronounced edema of the tissues of the upper lip and nose.
When the teeth are closed, the bony part of the nasal septum tends to move upward. Hemorrhage is determined in the tissue of the upper fornix of the vestibule of the mouth along the entire dentition. Often there is hemorrhage in the upper part of the pterygo-mandibular fold. The bite is broken. More often it is open, but it can be direct, progenic (if it was orthognathic before the injury), which depends on the severity and nature of the displacement of the fragments. If the fragment is not displaced, then the bite does not change. When the teeth are percussed, the percussion sound is low (dull). The soft palate is displaced posteriorly, and the small uvula touches the root of the tongue or the back of the pharynx. Palpation of the anterior and infratemporal surface of the upper jaw body can reveal a bony step
(protrusion) within the hemorrhage, i.e. along the entire perimeter of the jaw body. However, with a slight displacement of the fragment, when the periosteum does not rupture along the fracture gap, and also with severe post-traumatic edema and hematoma, it is quite difficult to palpate the step. This sign can be more clearly identified even with a slight displacement of the fragment in the area of the zygomatic alveolar ridge, since its profile is sufficiently well contoured.
The painful symptom of the load is positive: pressure on the hooks of the pterygoid processes of the sphenoid bone on both sides, the last molars or the hard palate is accompanied by painful sensations along the fracture gap. Sometimes in this case, the frontal section of the fragment goes down. This sign is of great diagnostic value, since it is positive even in the absence of clearly defined bony protrusions in typical places.
To determine the pathological mobility of the fragment, one should use the fingers of the right hand, grabbing the alveolar ridge in the frontal part, and gently (no more than 1-2 mm) move the alleged fragment back and forth. The index and thumb of the left hand, located on the left and right in the area of the alleged fracture gap, where the bony protrusion is palpated (more reliably - in the area of the zygomatic alveolar ridges), one can feel the mobility of the fragment. At the same time, a fold is often formed on the skin part of the nasal septum due to its connection with a broken bone frame, or the color of the skin in this place changes due to a change in the degree of tension of the soft tissues.
By pricking the mucous membrane of the gums with a sterile injection needle, one can make sure that there is no or a decrease in its pain sensitivity within all the teeth of the upper jaw. This is due to trauma to the anterior, middle and posterior alveolar branches of the infraorbital nerve, passing through the walls of the upper jaw.
A fracture of the upper jaw of the lower type should be differentiated from a fracture of the lateral alveolar process of the upper jaw. The painful symptom of loading, carried out according to the method described above (pressure on the pterygoid processes) with a fracture of the alveolar process will be negative, and on the large molars, it will be accompanied by pain in its zone. In this case, hemorrhage into the upper fornix of the vestibule of the mouth will be on one side, and there is no mobility of the upper jaw when trying to move it.
On the radiograph of the bones of the facial skeleton in the anterior semi-axial projection in the vertical position of the patient, the violation of the integrity of the walls of the pear-shaped opening and the zygomatic alveolar ridge on the left and right, as well as the level of fluid in the maxillary sinuses due to hemorrhage in them, is determined.
3. Asymmetrical fractures of the upper jaw.3.1. Unilateral fracture of the upper jaw.
In the practice of a dental surgeon, there are unilateral or sagittal fractures of the upper jaw. They often occur when the wounding object has no sharp edges and its force is directed from top to bottom in an oblique direction, mainly on the lateral part of one upper jaw or the upper lip area on one side. In this case, the body of the upper jaw breaks with the pterygoid process of the sphenoid bone of the corresponding side or without it. In the area of the anterior and infratemporal walls of the upper jaw, the fracture gap extends above the bottom of the maxillary sinus, and in the area of the hard palate - lateral to the median suture. In the midline of the hard palate, the fracture gap never passes. In this zone, it can have a zigzag or linear shape.
Thus, with this type of fracture, two bone fragments of unequal size are formed, represented by a broken upper jaw on one side and an intact one on the other. Each of them includes the upper jaw, palatine bone
(as a component of the hard palate) and the pterygoid process of the sphenoid bone. The nasal septum is connected to the intact upper jaw. However, it can break if the fracture gap crosses the midline. The broken off fragment is displaced downward and posteriorly - the action of the applied force and traction of the medial pterygoid muscle, as well as outward - the action of the fibers of the lower head of the lateral pterygoid muscle, attached to the outer surface of the pterygoid process of the sphenoid bone. This causes malocclusion.
With a unilateral fracture (say, on the right), patients complain of pain in the right upper jaw, aggravated by closing the teeth or trying to chew food, the inability to close the teeth correctly, numbness of all the teeth and gums of the upper jaw on the right, and sometimes a feeling of a foreign body in the throat.
On examination, one-sided (right) deformity of the face is determined due to edema of the tissues of the upper lip, buccal and infraorbital regions. There may be hemorrhages in the indicated areas, abrasions, wounds - traces of the applied force. The patient's mouth is half-open. The mucous membrane of the alveolar process between the central incisors (or the central and lateral incisors on the right) is torn. There is hemorrhage in the upper fornix of the vestibule of the mouth and above it on the side of the fracture within all the teeth. The bony protrusion is palpated within the hematoma, including in the area of the zygomatic alveolar ridge. On the hard palate - pronounced hemorrhage, often - a laceration of the mucous membrane.
Sometimes the divergence of fragments is so great that the wound resembles a congenital cleft of the hard palate, through which the nasal cavity is visible.
When pressing on the pterygoid process of the sphenoid bone or the last molars, the mobility of the fragments is visually revealed, as well as during palpation control in the area of the zygomatic alveolar ridge.
The teeth between which the fracture gap passes can be mobile. Their percussion is moderately painful, the percussion sound is low. The teeth are in contact on the side of the fracture. In this case, a more dense contact of the palatine tubercles of the teeth of the upper jaw with the buccal tubercles of the teeth of the lower jaw is determined. There are no teeth on the healthy side.
The symptom of mobility of fragments is positive.
On the radiograph of the upper jaw in the anterior semi-axial projection, there is a decrease in the transparency of the right maxillary sinus, a violation of the integrity of the zygomatic alveolar ridge on this side.
On the radiograph of the hard palate, a fracture gap is visible.
3.2. Fracture of the upper jaw of the Le Fort I type on one side and Le Fort II on the other.
For the convenience of presenting the material, we will assume that on the left the fracture gap passes along the upper type, and on the right - along the middle one. The fracture line begins at the junction of the frontal process of the upper jaw with the nasal part of the frontal bone. On the left, it spreads characteristic of a Le Fort I fracture, and on the right, Le Fort II (Fig. 25).
The patient may complain of pain in the upper jaw, aggravated by closing the teeth or trying to bite off or chewing food, improper closing of the teeth, sensation of a foreign body in the throat, choking and retching, insufficiently wide opening of the mouth, double vision. On the right, there may be numbness of the skin of the lower eyelid, infraorbital region, wing of the nose, incisors, canine teeth, premolars and mucous membrane of the gums from the vestibular side in the area of these teeth. On the left - numbness of the skin of the upper eyelid, forehead, outer and inner corner of the palpebral fissure (in case of damage to the orbital nerve in the area of the supraorbital fissure).
The face is deformed due to post-traumatic edema and subcutaneous emphysema on the right. When the patient is transferred to a vertical position, the process of lengthening the face is noticeable, and when transferred to a horizontal position, its shortening and flattening. Possible two-
 Rice. 25. Scheme of an asymmetric fracture of the upper jaw of the Le Fort I type on the left
Rice. 25. Scheme of an asymmetric fracture of the upper jaw of the Le Fort I type on the left
and Le Fort II on the right.
third-party exophthalmos due to hemorrhage in retrobulbar tissue. Hemorrhage in the soft tissues of the periorbital zone is determined: on the left - typical for the upper, and on the right - for the middle type. When the teeth are closed, the eyeball on the left can move upward, the palpebral fissure can narrow. At the same time, doubling in the eyes may decrease, a skin fold appears in the area of the root of the nose.
On palpation of the facial skeleton, a bony protrusion is determined in the region of the upper outer corner of the orbit and the zygomatic arch on the left, the infraorbital margin on the right, as well as a bony protrusion at the nasal part of the frontal bone, or there is a feeling of tissue falling under the finger in this zone (with pronounced displacement of fragments). When determining the symptom of the mobility of the bone fragment under the fingers of the left hand, it is possible to determine the mobility of the fractured fragment in the region of the infraorbital edge on the right, the upper outer corner of the orbit and the zygomatic arch on the left, as well as in the region of the root of the nose. The opening of the mouth is somewhat limited.
The bite is open (or straight). In the absence of displacement, the ratio of the teeth may not change. On the right, along the transitional fold of the upper jaw, within the premolars and molars, hemorrhage is clearly visible, extending to the mucous membrane of the cheek. On palpation of the anterior and infratemporal surface of the body of the upper jaw, a bony protrusion is palpated in the area of the zygomatic alveolar ridge to the right and behind it. On the left, these signs cannot be found. Reduced pain sensitivity of the mucous membrane of the gums, respectively, the frontal group of teeth on the right. In the upper part of the pterygo-mandibular fold, there may be hemorrhage on the right, but there is no hemorrhage on the left side. The soft palate is displaced posteriorly, and the small uvula may touch the back of the pharynx or the root of the tongue. With percussion of the teeth - a low percussion sound.
On radiographs - a decrease in the transparency of the maxillary sinuses, a violation of the integrity of the bone tissue: on the left - in the area of the root of the nose, fronto-zygomatic suture and zygomatic arch, on the right - in the area of the infraorbital margin and zygomatic alveolar ridge.
With this variant of a fracture of the upper jaw, a fracture of the base of the skull is possible with no less probability than with a symmetrical fracture of the upper or middle type. In this case, the radiograph may show a step or fracture line located on the Turkish saddle or somewhat anterior to it.
3.3. Upper jaw fracture as Le Fort II on one side and Le Fort III - with
another.
Suppose that the fracture on the left is in the middle, and on the right, in the lower type. The fracture line, starting at the junction of the frontal process of the upper jaw with the nasal part of the frontal bone on the left, extends along the inner wall of the orbit and further in accordance with the Le Fort II fracture, but only on one left side. Unlike the classical (symmetrical) version, the nasal septum may be intact, because will be completely located on the other (right) upper jaw. On the right, the fracture line, starting at the pear-shaped opening, spreads characteristic of a fracture of the lower type (Fig. 26).
The patient complains of pain in the upper jaw, aggravated by closing the teeth and trying to chew food; improper closing of teeth; sensation of a foreign body in the throat, retching; numbness of the skin of the infraorbital region, lower eyelid, wing and skin part of the nasal septum on the left; numbness of all teeth and gingival mucosa within these teeth on the right; numbness or decreased pain sensitivity in the area of incisors, canine and premolars on the left and gum tissue within these teeth; double vision when looking to the side.
 Rice. 26. Scheme of asymmetric fracture of the upper jaw according to Le Fort II on the left
Rice. 26. Scheme of asymmetric fracture of the upper jaw according to Le Fort II on the left
and Le Fort III on the right.
On examination, deformity of the face is determined due to post-traumatic edema of tissues: on the left - mainly in the infraorbital, zygomatic, buccal region, on the right - in the buccal and upper lip region. On the left, there may be a hemorrhage in the tissue of the infraorbital region, upper and lower eyelids, the inner corner of the orbit, the root of the nose, the conjunctiva and in the sclera of the eyeball. With severe hemorrhage in retrobulbar tissue - exophthalmos. However, unilateral enophthalmos on the left is possible. There may be abrasions, wounds, bruises of various localization, both on the left and on the right.
On palpation of the infraorbital margin on the left and the area of the root of the nose, a bony protrusion or tissue retraction can be determined. In some patients, a bone step is palpable in the region of the lower outer corner of the orbit, i.e. the fracture gap passes through the zygomatic bone and the bottom of the orbit and, together with the upper jaw and eyeball, moves downward. This leads to a violation of the alignment of the eyeballs, which is manifested in patients with diplopia.
When applying painful irritations with a needle, there is a lack or decrease in pain sensitivity of the skin of the infraorbital region, lower eyelid, wing and skin part of the nasal septum. With a significant posterior displacement of the fragments, a one-sided flattening of the face (on the left) is possible, but less pronounced than with a symmetric fracture of the middle type. On the upper fornix of the vestibule of the mouth, there is hemorrhage within all the teeth on the right and molars on the left. The bite is often open, but it can also be direct. Pain sensitivity of the gingival mucosa is reduced or absent in the area of all teeth on the right and incisors, canine and premolars on the left.
On palpation, a bony step is determined within the infratemporal and anterior walls of the upper jaw on the right and the infratemporal wall on the left. It can be especially clearly defined in the area of the zygomatic alveolar ridge, both on the left and on the right.
The soft palate is displaced posteriorly, in the upper parts of the pterygo-mandibular folds (left and right) there may be hemorrhage. When trying to displace a bone fragment, mobility is determined in the area of the zygomatic alveolar ridge on the left and right, the infraorbital edge on the left and the root of the nose. The formation of a skin fold in the area of the root of the nose and the skin part of its septum is possible. The symptom of the load is positive and is manifested by painful sensations on the left and on the right, not symmetrically, but in accordance with the location of the fracture gap. When percussion of the teeth, both left and right, a dull sound is determined. With this type of fracture, there are frequent signs of a fracture of the base of the skull and brain injury.
On the radiograph of the upper jaw in the anterior semi-axial projection, a decrease in the transparency of the maxillary sinuses on the left and on the right is determined, a violation of the integrity of the zygomatic alveolar ridge on both sides, the infraorbital margin on the left.
3.4. Tab. 1: Differential diagnosis of non-fire displaced maxillary fractures
 Continuation of table 1.
Continuation of table 1.
 End of table 1.
End of table 1.
 Note: (+) - the feature is always determined, (+ -) - the feature can be sometimes, (-) - the feature is never determined
Note: (+) - the feature is always determined, (+ -) - the feature can be sometimes, (-) - the feature is never determined
Upper jaw is a paired bone, but both halves of it are welded together along the midline very firmly, so that in most cases it breaks like one bone in the event of injury. The fracture line often affects both sides of the bone. The upper jaw is built of rather thin bony plates, which are the walls of the maxillary sinus located inside the bone, lined with mucous membrane. The upper jaw is firmly fused with other bones of the facial skeleton with the help of bone sutures and participates in the formation of the oral cavity, nose, orbit, as well as the infratemporal and pterygopalatine fossae. In the posterior section, it is fused with the bones of the base of the skull.
Upper jaw takes a deeper position among the bones of the facial skeleton. The anterior part of the alveolar process of the jaw is less protected from impacts, so its fractures are quite common and account for 60% of all fractures of the upper jaw. Due to the strong connection of the upper jaw with the adjacent bones, very often with its fracture, other bones of the face, and sometimes the base of the skull, are fractured at the same time.
Upper jaw, like the lower one, has several weak areas, in which fractures usually occur with trauma. Fractures in these places are called Le Forum fractures. There are three types of such fractures.
First type(Le Fort-1) - the fracture line passes transversely through the root of the nose, then goes to the medial wall of the orbit to the inferior orbital fissure, from here it goes to the lower edge of the orbit at the junction of the upper jaw with the zygomatic bone. Then it goes through the anterior wall and the outer edge of the orbit and posteriorly passes through the pterygoid process of the main bone, also causing a fracture of the zygomatic arch. With this fracture, there is a complete separation of the upper jaw with the nasal and zygomatic bones from the base of the skull. Such a fracture is called complete craniofacial separation.
Second type(Le Fort-2) - the fracture line passes transversely through the root of the nose, then goes to the medial wall of the orbit to the inferior orbital fissure, from here it goes to the lower edge of the orbit at the junction of the upper jaw with the zygomatic bone. The fracture line passes through the nasal septum and through the ends of the pterygoid processes of the main bone. In this fracture, the upper jaw, along with the nasal bones, is separated from the zygomatic bone and skull bones. Such a fracture is accompanied by hemorrhage in the eyelids and conjunctiva, sometimes there are bleeding from the mouth, nose and nasopharynx. Often, these fractures are combined with fractures of the ethmoid bone, accompanied by a concussion of the brain and even the formation of cracks in the base of the skull.
Third type(Le Fort-3) - the fracture line runs horizontally over the alveolar process from the base of the piriform foramen to the lesser pterygoid process of the main bone. In this case, the bottom of the maxillary sinus usually breaks off and the nasal septum breaks.
Often with traumatic fractures of the upper jaw the above fracture lines are located asymmetrically: on the one hand - along the second type, on the other - along the first. There are also unilateral fractures of the upper jaw, when the fracture line does not go beyond the midline. In these patients, one half of the upper jaw is separated from the other in the midline.
Please note that the above scheme of fractures of the upper jaw according to Le Forum do not cover all possible variants of fractures of this bone of the facial skeleton. There may be fractures of one half of the jaw with significant fragmentation of the bone, comminuted, etc. Due to the strong anatomical and physiological connection of the upper jaw with the base of the cerebral skull, fractures and cracks of the orbital bones, ethmoid bone, as well as combinations with a fracture of the sella turcica, large or small pterygoid processes of the main bone, the clivus of the occipital bone and the stony part of the temporal bone.
With a fracture of the upper jaw the victims complain of a headache, the inability to clench their jaws, indicate a crunch when the fragments move. In some cases, upon examination, attention is drawn to a significant swelling of the middle part of the face, sometimes with hemorrhage under the lower eyelids and at the inner corners of the eyes, there may be hemorrhages in the sclera of the eyeball. In other cases, a retraction of the middle part of the face is revealed, which indicates a posterior displacement of the fragments of the upper jaw. At the same time, with a fracture of the nasal bones and the septum of the moequette, there is a deformation of the nasal dorsum.
When examining the oral cavity more often you can find a violation of the bite. When the fragments are displaced posteriorly, there is an open bite, when displaced downward, the fragment of the moeket hangs on the peri-maxillary soft tissues and freely moves forward. With hemorrhages in the retrobulbar tissue, protrusion of the eyeball (exophthalmos) is observed. Damage to the maxillary sinus is sometimes accompanied by subcutaneous emphysema on the corresponding side of the face. In severe cases, emphysema moeket spread to the neck.
If the fragments are displaced and squeeze the infraorbital nerve, there is pain in the infraorbital foramen area. With a complete rupture of the infraorbital nerve, anesthesia is observed in the region of the upper lip and wing of the nose on the corresponding side. With traumatic nerve damage in the canal, even before it leaves the infraorbital opening, anesthesia of the teeth occurs on the corresponding half of the upper jaw. If the fracture of the upper jaw is combined with a fracture of the wing of the main bone, pain when swallowing is possible. On palpation of the surface of the face, it is possible to determine the mobility of the fragment, accompanied by sharp pain. Palpation of the upper jaw from the side of the oral cavity reveals the mobility of bone fragments more clearly.
With a punctured fracture, including a bone fragment of the base of the skull, pathological mobility cannot be determined. Malocclusion and the presence of other symptoms described above make it possible to diagnose a fracture with sufficient accuracy and establish its nature. X-ray of the bones of the facial skull in frontal and lateral projections helps to clarify the fracture line, its location and nature.
Content of the article: classList.toggle () "> expand
Skull fractures pose a serious threat to human health. As a result of such an injury, a dangerous complication (for example, meningitis or concussion) can occur, which is fraught with disability in the future.
In the vast majority of cases, the fracture of the upper jaw occurs as a result of traffic accidents, fights, falls from a height, etc.
Anatomical features of the structure of the upper jaw
To understand the specifics of the injury, you need to know the structural features of the upper jaw. So, the upper jaw is a paired bone, which has connections with several bones of the facial skull: sphenoid, ethmoid, zygomatic, frontal and nasal. In the places of their joints, the so-called bone sutures are formed.
It is in the places of the bone sutures that the fracture lines pass. This is due to the fact that these areas have less strength and are easily injured by mechanical stress.
In addition, the presence of bone sutures on the facial skull determines the combined nature of the injury. An isolated fracture of the upper jaw is rare, more often it spreads to adjacent bones.
The second anatomical feature of the upper jaw is the abundance of blood vessels. Therefore fractures are accompanied by intense bleeding... Moreover, trauma is characterized by both external and internal bleeding. The latter have an unfavorable prognosis: firstly, such bleeding cannot always be detected in a timely manner, and secondly, technical difficulties often arise during its stopping.
Fracture classification
There are several classifications of maxillary fractures. Complete and incomplete (depressions, cracks, breaks).
Depending on the cause of the occurrence:
- Traumatic (resulting from the impact of a mechanical factor, for example, shock). In turn, they are divided into firearms and non-firearms.
- Pathological. A pathological fracture of the upper jaw occurs as a result of bone disease (syphilis, osteomyelitis, tuberculosis, etc.).
Depending on the preservation of soft tissues:
- Closed;
- Open.
By the mechanism of fracture:
- Straight lines - arise at the site of application of the traumatic factor;
- Indirect - arise at a distance from the place of exposure to the traumatic factor.
Displacement fracture
The displacement of the bones of the upper jaw with a fracture can be of several types:
- Displacement back, that is, in the direction of the traumatic force;
- Downward displacement, that is, under the action of their own gravity and muscle traction. In this case, the displacement will be uneven, since the posterior parts of the upper jaw are displaced to a greater extent than the anterior ones. This feature is due to the traction of the pterygoid muscle.
The type of displacement largely determines the tactics of further treatment and the timing of rehabilitation.
The nature of the displacement of bone fragments also depends on the fracture line. It can be oblique, transverse, straight, zigzag, etc.
In clinical practice, the sagittal type of fracture of the upper jaw is also distinguished. This term is called a fracture of one of the bones of the upper jaw. It was mentioned above that the upper jaw is a paired bone.
Maxillary fractures according to Lefort classification
From a practical point of view, the most convenient is the classification of fractures of the upper jaw, proposed in 1901 by Lefort. Lefort identified 3 types of fracture:
- Lefort I, or upper (in the picture below - a). Represents an incomplete transverse fracture. Its line runs horizontally. This breaks off the bottom of the nose and the bottom of the maxillary (maxillary) sinus. If the fracture is bilateral, then a horizontal fracture of the nasal septum will occur. Often Lefort I is accompanied by neurological symptoms.
- Lefort II, or medium (in the picture below - b). The fracture line passes through the bones of the nose, the inner surface of the orbit. In this case, the nasal septum breaks in the vertical direction. The cause of such an injury is a powerful blow to the nose with closed jaws.
- Lefort III, or lower (in the picture below - c). With this fracture, the entire jaw (together with the zygomatic processes) is separated from the base of the skull. It is considered the most unfavorable type of fracture. It is accompanied by concussion, bruising or compression of the brain.

Situations are not uncommon when mixed fractures occur (for example, both Lefort I and Lefort II).
Damage mechanism
The fracture of the upper jaw occurs as a result of a strong and rough effect of a mechanical factor (fall from a height, blow to the face, compression, etc.). In this case, the displacement of bone fragments occurs. The nature of the displacement depends on several factors. The first is the traction force of the lateral (lateral) pterygoid muscles, which causes lateral displacement of the bones. The second factor is the gravity of the bones, which moves the bones downward.
During a strong compression of the jaw between two objects, the displacement of the jaw bones is accompanied by a displacement of the bones of the nose and cheekbones, as well as ruptures of soft tissues. Sometimes the jaws diverge in different directions.
Often, as a result of a fracture, damage to the paranasal sinuses occurs, as a result of which subcutaneous emphysema may occur. This is a condition in which air bubbles penetrate the subcutaneous tissue.
Upper jaw fracture symptoms
The clinical picture of a fracture of the upper jaw is very diverse and largely depends on the type of fracture (signs of fracture Lefort I, II and III differ from each other).
A fracture is characterized by the following symptoms:
- Sharp pain. The epicenter of pain is located directly at the site of exposure to the traumatic factor, and from it can spread to all parts of the skull. Increased pain occurs even with the smallest attempt to open the mouth.
- Change in the relief of the face in the area of the fracture. The severity of this symptom depends on the degree of bone displacement.
- Bleeding. This symptom accompanies almost any type of jaw fracture. The danger of bleeding lies in the fact that they can be not only external, but also internal. As a result, it is not always possible to adequately assess the degree of blood loss.
- Increasing edema of the face, often with the formation of subcutaneous hematomas. For complicated fractures, accompanied by trauma to the base of the skull, the symptom of "glasses" is characteristic - a hematoma around the eyeballs.
- Neurological symptoms (dizziness, unsteadiness of gait, meningeal signs, etc.).
Diagnostics
Diagnosis of a fracture of the upper jaw begins with questioning the patient (if he is, of course, conscious) and examination. Inspection data often make it possible to establish the nature of the fracture and the presence of possible complications.
Radiological diagnostic methods are the gold standard for diagnosing any fracture, including injuries of the upper jaw. For uncomplicated injuries, the study begins with a conventional X-ray. This is a simple, inexpensive and painless technique for the patient, which shows not only the presence of a fracture, but also its nature, the presence of displacements, the number of fragments, etc. The picture must be taken in 2 projections.
 In the case of serious injuries, especially with craniocerebral trauma, it is necessary to resort to more informative diagnostic methods:
In the case of serious injuries, especially with craniocerebral trauma, it is necessary to resort to more informative diagnostic methods:
- Spiral computed tomography. Lets you get a layered image of bones. The undoubted advantage of the method is the high accuracy and detail of all elements.
- Magnetic resonance imaging (MRI). Provides detailed information about soft tissue damage.
- Orthopantomography. Using this method, you can get a panoramic image of the dentition.
First aid for fracture of the upper jaw
The outcome of the treatment of facial injuries is highly dependent on the timeliness and correctness of first aid. It is important to remember that the appearance of the victim and the visible damage do not always correspond to the true severity of the condition. For example, as a result of an injury, profuse internal bleeding may develop, which will not be noticed by others.
First aid includes several important activities:
- Prevention of asphyxia (suffocation). To avoid this formidable complication, you need to give the victim a special position: sit down with a slightly tilted body and head down. If a person is unconscious, you need to lay him on his back and turn his head to the side.
- Stopping bleeding. To stop bleeding from small vessels, it is enough to apply a pressure bandage to the damaged area. For the best effect, the dressing can be moistened with hydrogen peroxide, since this substance has a hemostatic (hemostatic) property. If the source of bleeding is large vessels (for example, branches of the carotid artery), then finger pressure should be applied to them. Do not use tight bandaging under any circumstances! This can cause displacement of bone fragments.
- Prevention of wound infection. In the vast majority of cases, fractures of the upper jaw are open, that is, the wound surface communicates with the environment. As a result, the risk of infection and the development of pyoinflammatory complications increases. To avoid this, you need to make a toilet of the wound: carefully clean it from contamination and treat it with any antiseptic solution. If you don't have anything at hand, you should at least close the wound with a clean dry napkin.
healthy
know!
Upper jaw fracture treatment
A maxillary fracture should be treated by a maxillofacial surgeon. In some situations, this function is taken over by traumatologists, dentists and ENT doctors.
Osteosynthesis
 One of the methods for treating a fracture of the upper jaw is osteosynthesis, during which bone fragments are fastened together with metal structures. The indications for osteosynthesis are as follows:
One of the methods for treating a fracture of the upper jaw is osteosynthesis, during which bone fragments are fastened together with metal structures. The indications for osteosynthesis are as follows:
- The presence of several bone fragments;
- Neoplastic process in the area of the fracture;
- Fractures located behind the dentition;
- Reconstructive interventions.
There are several types of osteosynthesis:
- Outer. In this case, metal wires are inserted perpendicular to the bony axis, which are subsequently attached to a special apparatus. Thus, the fracture site is relieved and the function of the upper jaw is partially restored.
- Extra bone osteosynthesis. It implies the imposition of a metal plate on the fracture area, which is attached to the bone with special screws and screws. This technique eliminates the imposition of plaster and promotes rapid recovery.
- Transosseous osteosynthesis. In this case, the metal structure is inserted into the bones at a certain angle so that the bone fragments are firmly fixed with each other.
Closed matching of fragments
There are situations when the reposition (juxtaposition) of bone fragments can be done in a closed way, that is, without resorting to surgical intervention. The main advantage of closed reduction is safety and minimal risk of injury. The disadvantage is the long-term external fixation of the jaw.
The method involves the application of a fixation splint on the upper jaw, which is attached to the teeth and, thus, stabilizes the bone fragments.
Bone suture
During this operation, soft tissues are exposed in the area of the fracture, after which several holes are made in the bone fragments. Subsequently, a wire (titanium or made of stainless steel) is passed through them, with which the bones are compared and tightly fixed. This technique is used if there is no strong displacement of the bones. Contraindications for performing a bone suture are:
- Osteomyelitis;
- Intense inflammatory process;
- Gunshot wound;
- The presence of multiple fragments.
The choice of the method of treatment is determined by the doctor individually, depending on the nature of the injury, the presence of concomitant diseases, as well as on the individual characteristics of the person.
Jaw fracture nutrition
With a fracture of the upper jaw, a person can consume exclusively liquid food, since he is unable to chew. As a result, the amount of nutrients coming from outside is reduced. This sometimes slows down the healing process.
When the upper jaw is fractured, there are several ways to feed:
- Physiological. It is available if the victim can open his mouth. Feeding is carried out using a cup, spoon or sippy cup with a rubber tube. The food is heated to 45-50 degrees and the patient is fed several times a day, until a feeling of complete satiety.
- Food with a gastric tube. This feeding method must be carried out by medical personnel, since it is necessary to have certain skills and knowledge to set the tube. Food is injected using a funnel or syringe at least 4 times a day. At the same time, breakfast should account for at least 30% of the daily volume, for lunch - 40%, for dinner - 20%, for the second dinner - 10%.
- If a person is unconscious, then his feeding is carried out by the parenteral route (bypassing the gastrointestinal tract). For this purpose, nutritional mixtures are administered intravenously.
 After discharge from the hospital, patients should strictly follow the recommendations of the attending physician regarding nutrition at home. First of all, the food should be liquid and contain a lot of nutrients and vitamins.
After discharge from the hospital, patients should strictly follow the recommendations of the attending physician regarding nutrition at home. First of all, the food should be liquid and contain a lot of nutrients and vitamins.
To give food a liquid consistency, it should be diluted with milk, vegetable or meat broth.... Vegetables included in the daily diet must be mashed.
You can use beets, cabbage, tomatoes, fresh herbs, carrots, potatoes, etc. Fermented milk products (milk, yogurt, sour cream, cottage cheese) are very useful, as they contain a lot of calcium, which is necessary for bone healing. It is imperative to use vegetable oils.
Recovery time after fracture
On average, the duration of temporary disability (sick leave for working citizens) with a fracture of the upper jaw is about 65 days. This figure can vary widely, as it depends on the type of injury.
Recovery after a Lefort I fracture takes, on average, about 56 days, after Lefort II - 65 days, and after Lefort III - about 75 days.
If there is a complicated fracture, then recovery can last for 3 months or more.
Rehabilitation after a fracture of the upper jaw complicated by a concussion lasts about 70 days. With a combination of a fracture of the upper and lower jaw, recovery lasts about 75 days; when combined with a fracture of the orbit - 120 days.
Recovery time is also influenced by the way the fracture is treated. With surgery, it is, on average, 76 days, and with orthopedic treatment of fractures of the upper jaw - 60 days.
Fracture recovery and lifestyle
To speed up bone healing, you need to take a comprehensive approach to rehabilitation measures and strictly follow all the doctor's prescriptions. Much attention should be paid to the methods of physiotherapy treatment, physiotherapy exercises, as well as regular oral hygiene.
Physiotherapy
The essence of physiotherapy methods is reduced to local effects physical factors(heat, vibration, infrared radiation, electrical impulses, etc.). In case of a fracture of the upper jaw, the following physiotherapy procedures are shown:
- UHF. This is the effect on the tissues of the electromagnetic field of ultra-high frequency. The procedure has a local warming effect, thereby increasing blood flow and metabolism. Additionally, the intensity of pain is reduced. The effect appears after 10 sessions.
- Magnetotherapy. Reduces the intensity of inflammation in the tissues and has an analgesic effect. 9-10 sessions are carried out.
- Electrophoresis. Delivery is possible with the help of electrophoresis mineral substances(in particular, calcium) deep into the tissues. This contributes to the acceleration of bone tissue regeneration. It is recommended to carry out 10-15 sessions.
Physiotherapy
Physiotherapy exercises (exercise therapy) plays an important role in the restoration of the function of the upper jaw. Before starting the exercises, you should definitely consult with a specialist. He will select an individual training program and monitor the correctness of certain exercises. The timing of when you can start exercise therapy is individual for each patient.
Fracture Oral Care
Oral hygiene plays an important role during rehabilitation. Food debris serves as a breeding ground for pathogenic microflora. This can cause an inflammatory reaction with the formation of abscesses. An additional aggravating factor is metal structures (knitting needles, wire) that fix bones and can cause pressure sores on the gums.
 Treatment of the oral cavity is carried out by medical personnel (during dressings) and by the patient himself. The following antiseptic solutions are used: 3% hydrogen peroxide solution, potassium permanganate solution, furacillin, chlorhexidine, etc.
Treatment of the oral cavity is carried out by medical personnel (during dressings) and by the patient himself. The following antiseptic solutions are used: 3% hydrogen peroxide solution, potassium permanganate solution, furacillin, chlorhexidine, etc.
Processing must be carried out with a syringe or rubber bulb. It is not recommended to use gauze or cotton balls, as their fibers will remain on metal structures.
It is important that the patient rinses his mouth not only after each meal, but also in between meals. Any food remains stuck between the teeth should be carefully removed with a toothpick.
In addition, you should regularly brush your teeth with a hygienic paste and a toothbrush. The absence of fetid odor from the mouth indicates that the treatment of the oral cavity is carried out correctly.
Complications and consequences
Complications that arise as a result of a fracture of the upper jaw can be divided into early and late. Early complications include:

Late complications:
- Formation of false joints.
- Osteomyelitis.
- Post-traumatic sinus inflammation (eg, sinusitis).
- Slow bone fusion.
- Deformation of the bones.
- Formation of contractures (persistent contractions) of mimic muscles, as a result of which the chewing function of the jaw suffers.
- Losing weight.
To prevent infectious and inflammatory complications, it is important to timely prescribe antibacterial drugs with a wide spectrum of action: cephalosporins, penicillins, fluoroquinolones, macrolides, etc. The choice of a specific antibiotic and the duration of its administration is determined by the attending physician
Fracture of the upper jaw in children
In children, a fracture of the upper jaw can occur as a result of falling from a height (for example, from a tree), during a fight, riding a swing, etc.
Almost a third of childhood fractures of the upper jaw are accompanied by a concussion. The danger of this condition is that at first it can proceed without any visible signs. Therefore, if you suspect an injury, you must immediately show the baby to a specialist.
One of the features of childhood fractures is a decrease in the strength of the jaw due to the rudiments of teeth that have not yet erupted. Because of this, abnormal growth of permanent teeth is possible in the future. That is why dispensary supervision is established for such children until the formation of a permanent bite.
Treatment of fractures of the upper jaw in children is usually conservative. The use of osteosynthesis is justified only in the presence of multi-splinter fractures, which is not so common in practice. Arched arches and peri-maxillary splints are successfully used to fix the bones.
As for the healing time, in childhood, rehabilitation takes, on average, from 30 to 45 days. On x-ray, bone fusion can be traced already on the 20th day.